

Contribution of the ELFG test in algorithms of non-invasive markers towards the diagnosis of significant fibrosis in chronic hepatitis C
- PMID: 23555619
- PMCID: PMC3605459
- DOI: 10.1371/journal.pone.0059088
Contribution of the ELFG test in algorithms of non-invasive markers towards the diagnosis of significant fibrosis in chronic hepatitis C
Abstract
Background and aims: We aimed to determine the best algorithms for the diagnosis of significant fibrosis in chronic hepatitis C (CHC) patients using all available parameters and tests.
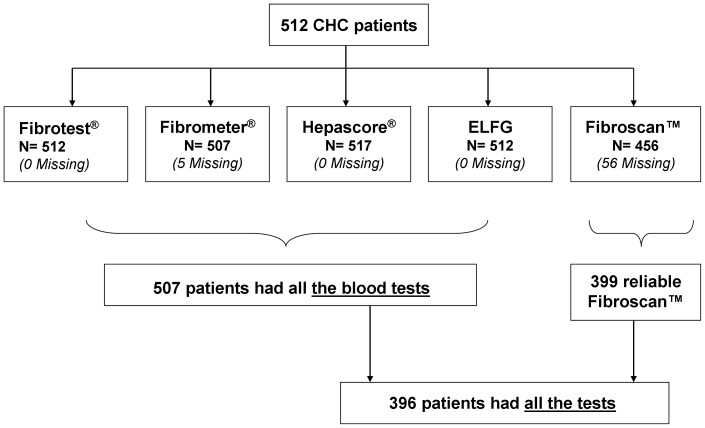
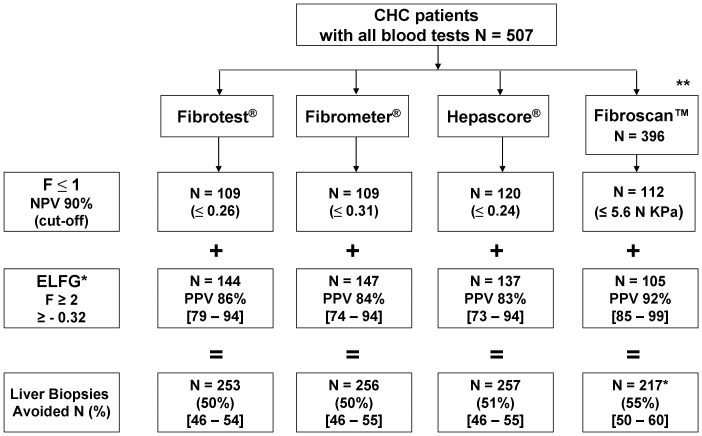
Patients and methods: We used the database from our study of 507 patients with histologically proven CHC in which fibrosis was evaluated by liver biopsy (Metavir) and tests: Fibrometer®, Fibrotest®, Hepascore®, Apri, ELFG, MP3, Forn's, hyaluronic acid, tissue inhibitor of metalloproteinase-1 (TIMP1), MMP1, collagen IV and when possible Fibroscan™. For the first test we used 90% negative predictive value to exclude patients with F≤1, next an induction algorithm was applied giving the best tests with at least 80% positive predictive value for the diagnosis of F≥2. The algorithms were computed using the R Software C4.5 program to select the best tests and cut-offs. The algorithm was automatically induced without premises on the part of the investigators. We also examined the inter-observer variations after independent review of liver biopsies by two pathologists. A medico-economic analysis compared the screening strategies with liver biopsy.
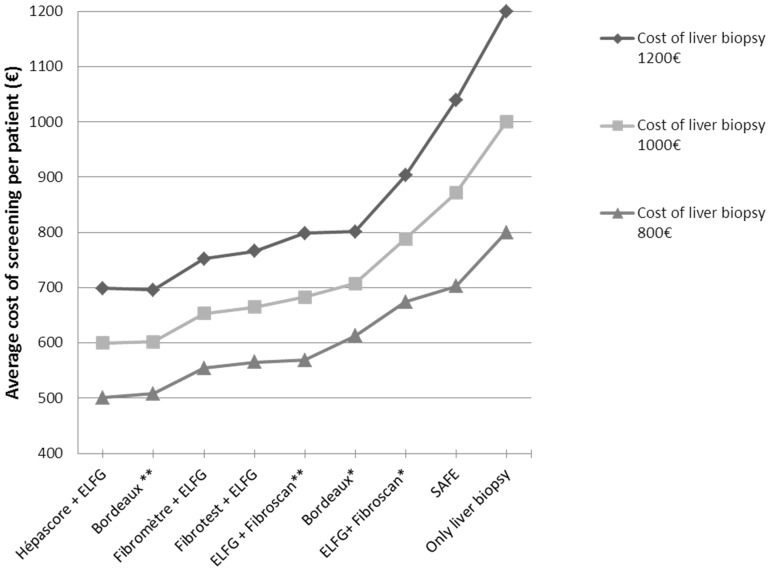
Results: In "intention to diagnose" the best algorithms for F≥2 were Fibrometer ®, Fibrotest®, or Hepascore® in first intention with the ELFG score in second intention for indeterminate cases. The percentage of avoided biopsies varied between 50% (Fibrotest® or Fibrometer®+ELFG) and 51% (Hepascore®+ELFG). In "per-analysis" Fibroscan™+ELFG avoided liver biopsy in 55% of cases. The diagnostic performance of these screening strategies was statistically superior to the usual combinations (Fibrometer® or Fibrotest®+Fibroscan™) and was cost effective. We note that the consensual review of liver biopsies between the two pathologists was mainly in favor of F1 (64-69%).
Conclusion: The ELFG test could replace Fibroscan in most currently used algorithms for the diagnosis of significant fibrosis including for those patients for whom Fibroscan™ is unusable.
Conflict of interest statement
Figures
References
-
- Adams L, Bulsara M, Rossi E, DeBoer B, Speers D, et al. (2005) Hepascore: an accurate validated predictor of liver fibrosis in chronic hepatitis C infection. Clin Chem 51: 1867–1873. - PubMed
-
- Cales P, Oberti F, Michalak S, Hubert-Fouchard I, Rousselet M-C, et al. (2005) A novel panel of blood markers to assess the degree of liver fibrosis. Hepatology 42: 1373–1381. - PubMed
-
- Imbert-Bismut F, Ratziu V, Pieroni L, Charlotte F, Benhamou Y, et al. (2001) Biochemical markers of liver fibrosis in patients with hepatitis C virus infection: a prospective study. Lancet 357: 1069–1075. - PubMed
-
- Ziol M, Handra-Luca A, Kettaneh A, Christidis C, Mal F, et al. (2005) Noninvasive assessment of liver fibrosis by measurement of stiffness in patients with chronic hepatitis C. Hepatology 41: 48–54. - PubMed
-
- Degos F, Perez P, Roche B, Mahmoudi A, Asselineau J, et al. (2005) Diagnostic accuracy of FibroScan and comparison to liver fibrosis biomarkers in chronic viral hepatitis: A multicenter prospective study (the FIBROSTIC study). J Hepatol 53: 1013–1021. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
