

Effectiveness of treatment with high-frequency chest wall oscillation in patients with bronchiectasis
- PMID: 23556995
- PMCID: PMC3623823
- DOI: 10.1186/1471-2466-13-21
Effectiveness of treatment with high-frequency chest wall oscillation in patients with bronchiectasis
Abstract
Background: High-frequency airway clearance (HFCWC) assist devices generate either positive or negative trans-respiratory pressure excursions to produce high-frequency, small-volume oscillations in the airways.HFCWC can lead to changes in volume of 15-57 ml and in flow up to 1.6 L/s, which generate minimal coughing to mobilize secretions. The typical treatment lasts 20-30 minutes, and consists of short periods of compression at different frequencies, separated by coughing.The aim of this study was to find the more efficacious treatment in patients with bronchiectasis: traditional techniques of chest physiotherapy (CPT) versus high frequency oscillation of the chest wall in patients with bronchiectasis.
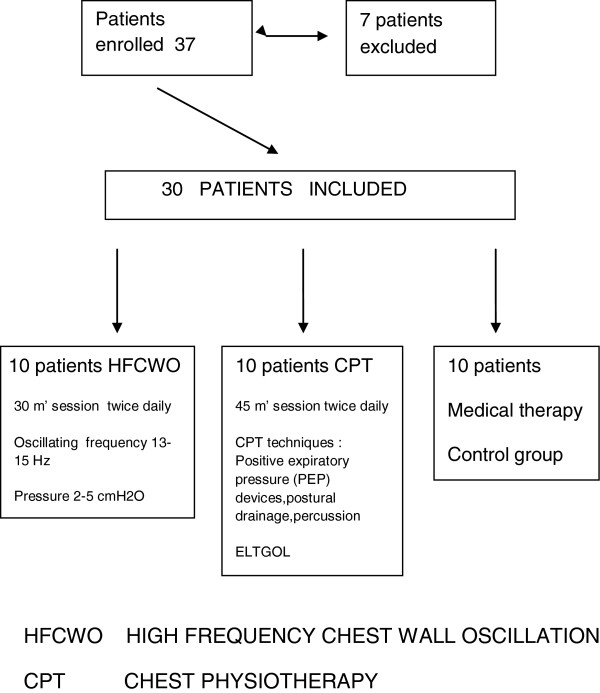
Methods: 37 patients were enrolled. Seven of them were excluded. Computer randomization divided the patients into three groups: - 10 patients treated with HFCWO by using the Vest® Airway Clearance System; - 10 patients treated with traditional techniques of air way clearance (PEP bottle, PEP mask, ELTGOL, vibratory positive expiratory pressure); - 10 patients received medical therapy only (control group). To be eligible for enrollment, participants had to be between 18 and 85 years old and have a diagnosis of bronchiectasis, confirmed on high resolution computed tomography.
Exclusion criteria: lack of informed consent, signs of exacerbation, cystic fibrosis. Before the treatment, each patient had blood tests, sputum volume and cell count, pulmonary function tests and on the quality of life inventories (MMRC, CAT, BCSS). The results were processed through the covariance analysis, performed with the R-Project statistical program. It has been considered a positive result p <005.
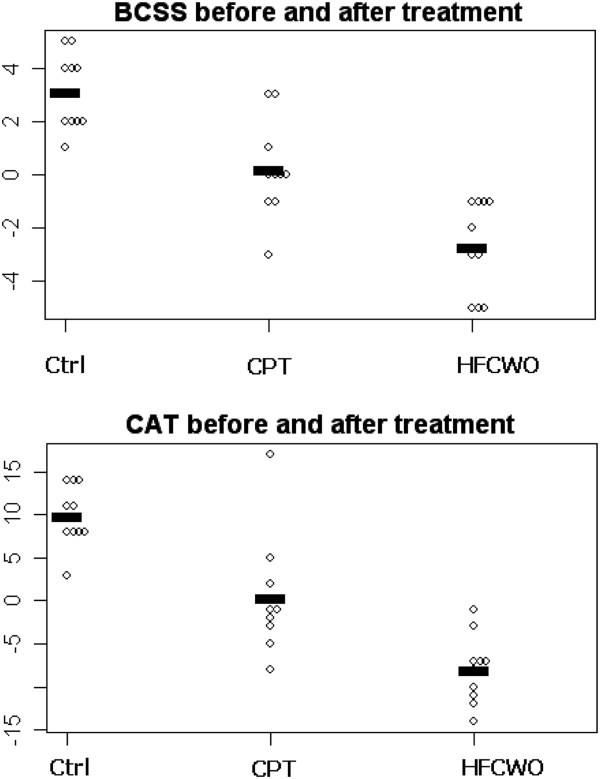
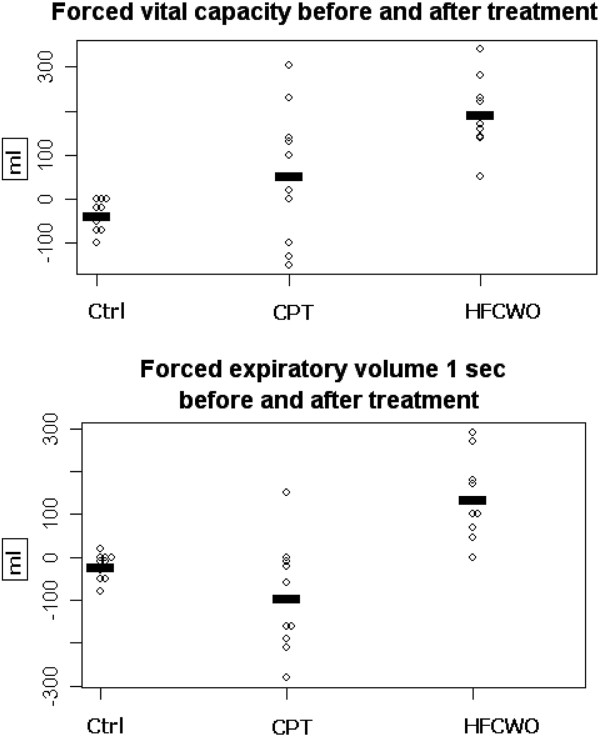
Results: Both treatments (traditional CPT and HFCWO) showed a significant improvement in some biochemical and functional respiratory tests as well as in the quality of life compared to the control group. The use of HFCWO compared to CPT also produced a significant improvement in blood inflammation parameter C-RP (p ≤0.019), parameters of lung functionality associated with bronchial obstruction (FVC, FEV1) (p ≤0.006 and p ≤0.001), and in the dyspnea. Improvement in quality of life scales was noted. (BCSS, CAT) (both p ≤0.001). No significant changes of total cell counts in sputum samples were observed in the two groups. In the HFCWO group a significant reduction of neutrophils percentage (p≤0.002) and a significant increase of macrophages percentage (p ≤0.012).
Conclusions: The HFCWO technique provides an improvement both in pulmonary function and quality of life related parameters in patients with chronic hypersecretive disease. Since those patients need daily airway clearance, this treatment should be included among the principal options in chest physiotherapy. The study was registered as ChiCTR-TRC-12002134 at http://www.chictr.org.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
