

HPV16 synthetic long peptide (HPV16-SLP) vaccination therapy of patients with advanced or recurrent HPV16-induced gynecological carcinoma, a phase II trial
- PMID: 23557172
- PMCID: PMC3623745
- DOI: 10.1186/1479-5876-11-88
HPV16 synthetic long peptide (HPV16-SLP) vaccination therapy of patients with advanced or recurrent HPV16-induced gynecological carcinoma, a phase II trial
Abstract
Background: Human papilloma virus type 16 (HPV16)-induced gynecological cancers, in particular cervical cancers, are found in many women worldwide. The HPV16 encoded oncoproteins E6 and E7 are tumor-specific targets for the adaptive immune system permitting the development of an HPV16-synthetic long peptide (SLP) vaccine with an excellent treatment profile in animal models. Here, we determined the toxicity, safety, immunogenicity and efficacy of the HPV16 SLP vaccine in patients with advanced or recurrent HPV16-induced gynecological carcinoma.
Methods: Patients with HPV16-positive advanced or recurrent gynecological carcinoma (n = 20) were subcutaneously vaccinated with an HPV16-SLP vaccine consisting of a mix of 13 HPV16 E6 and HPV16 E7 overlapping long peptides in Montanide ISA-51 adjuvant. The primary endpoints were safety, toxicity and tumor regression as determined by RECIST. In addition, the vaccine-induced T-cell response was assessed by proliferation and associated cytokine production as well as IFNγ-ELISPOT.
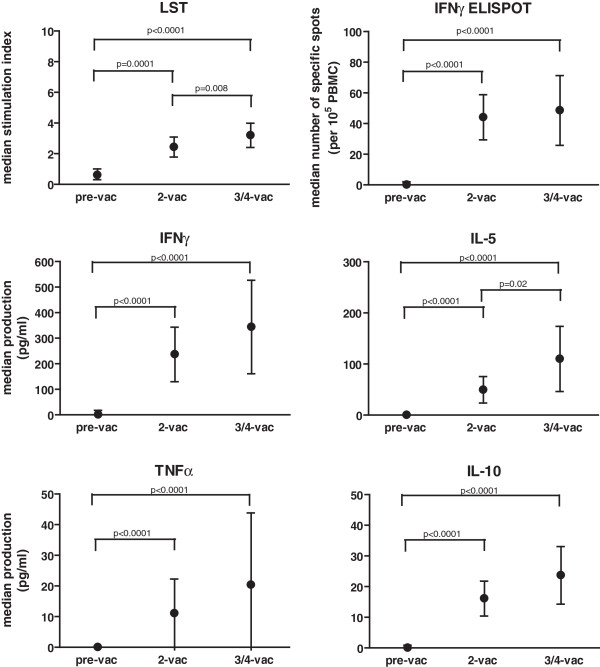
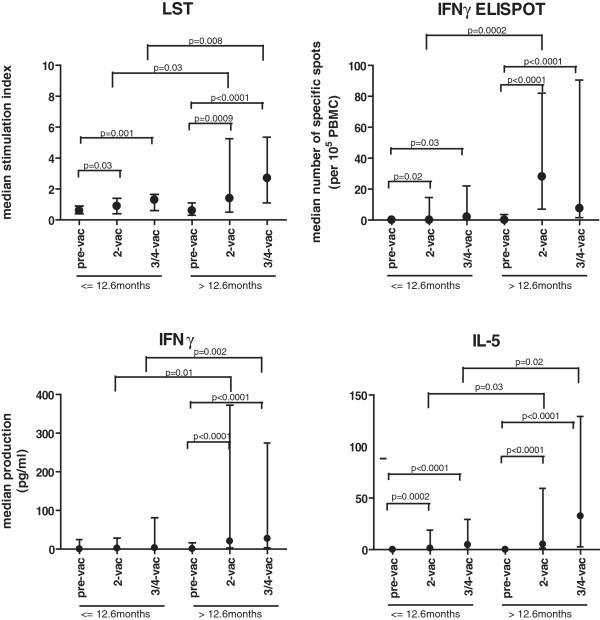
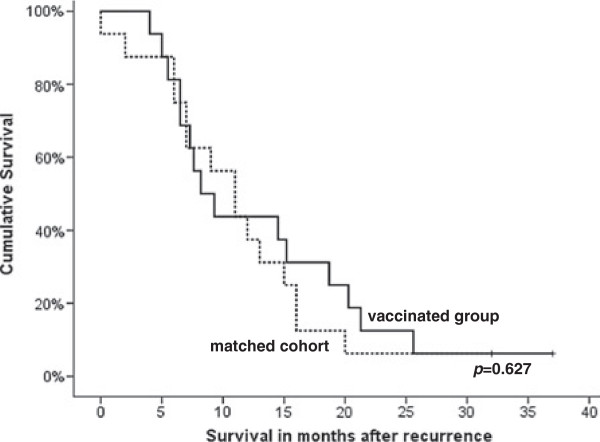
Results: No systemic toxicity beyond CTCAE grade II was observed. In a few patients transient flu-like symptoms were observed. In 9 out of 16 tested patients vaccine-induced HPV16-specific proliferative responses were detected which were associated with the production of IFNγ, TNFα, IL-5 and/or IL-10. ELISPOT analysis revealed a vaccine-induced immune response in 11 of the 13 tested patients. The capacity to respond to the vaccine was positively correlated to the patient's immune status as reflected by their response to common recall antigens at the start of the trial. Median survival was 12.6 ± 9.1 months. No regression of tumors was observed among the 12 evaluable patients. Nineteen patients died of progressive disease.
Conclusions: The HPV16-SLP vaccine was well tolerated and induced a broad IFNγ-associated T-cell response in patients with advanced or recurrent HPV16-induced gynecological carcinoma but neither induced tumor regression nor prevented progressive disease. We, therefore, plan to use this vaccine in combination with chemotherapy and immunomodulation.
Figures
References
-
- Burke TW, Hoskins WJ, Heller PB, Shen MC, Weiser EB, Park RC. Clinical patterns of tumor recurrence after radical hysterectomy in stage IB cervical carcinoma. Obstet Gynecol. 1987;69:382–385. - PubMed
-
- Zur Hausen H. Papillomavirus infections - a major cause of human cancers. Biochim Biophys Acta. 1996;1288:F55–F78. - PubMed
-
- Bosch FX, Manos MM, Munoz N, Sherman M, Jansen AM, Peto J, Schiffman MH, Moreno V, Kurman R, Shah KV. Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International biological study on cervical cancer (IBSCC) Study Group. J Natl Cancer Inst. 1995;87:796–802. doi: 10.1093/jnci/87.11.796. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
