

Clinical outcomes of patients requiring ventilatory support in Brazilian intensive care units: a multicenter, prospective, cohort study
- PMID: 23557378
- PMCID: PMC3672504
- DOI: 10.1186/cc12594
Clinical outcomes of patients requiring ventilatory support in Brazilian intensive care units: a multicenter, prospective, cohort study
Abstract
Introduction: Contemporary information on mechanical ventilation (MV) use in emerging countries is limited. Moreover, most epidemiological studies on ventilatory support were carried out before significant developments, such as lung protective ventilation or broader application of non-invasive ventilation (NIV). We aimed to evaluate the clinical characteristics, outcomes and risk factors for hospital mortality and failure of NIV in patients requiring ventilatory support in Brazilian intensive care units (ICU).
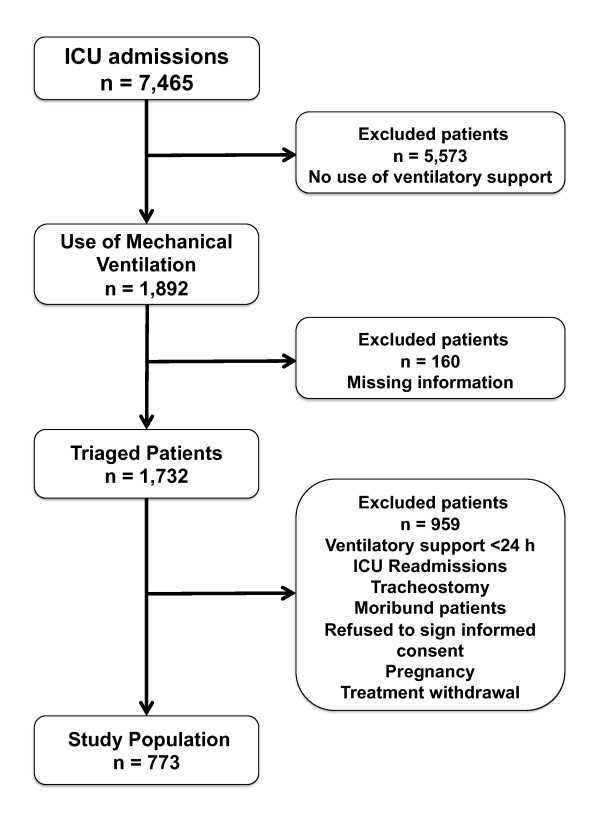
Methods: In a multicenter, prospective, cohort study, a total of 773 adult patients admitted to 45 ICUs over a two-month period requiring invasive ventilation or NIV for more than 24 hours were evaluated. Causes of ventilatory support, prior chronic health status and physiological data were assessed. Multivariate analysis was used to identifiy variables associated with hospital mortality and NIV failure.
Results: Invasive MV and NIV were used as initial ventilatory support in 622 (80%) and 151 (20%) patients. Failure with subsequent intubation occurred in 54% of NIV patients. The main reasons for ventilatory support were pneumonia (27%), neurologic disorders (19%) and non-pulmonary sepsis (12%). ICU and hospital mortality rates were 34% and 42%. Using the Berlin definition, acute respiratory distress syndrome (ARDS) was diagnosed in 31% of the patients with a hospital mortality of 52%. In the multivariate analysis, age (odds ratio (OR), 1.03; 95% confidence interval (CI), 1.01 to 1.03), comorbidities (OR, 2.30; 95% CI, 1.28 to 3.17), associated organ failures (OR, 1.12; 95% CI, 1.05 to 1.20), moderate (OR, 1.92; 95% CI, 1.10 to 3.35) to severe ARDS (OR, 2.12; 95% CI, 1.01 to 4.41), cumulative fluid balance over the first 72 h of ICU (OR, 2.44; 95% CI, 1.39 to 4.28), higher lactate (OR, 1.78; 95% CI, 1.27 to 2.50), invasive MV (OR, 2.67; 95% CI, 1.32 to 5.39) and NIV failure (OR, 3.95; 95% CI, 1.74 to 8.99) were independently associated with hospital mortality. The predictors of NIV failure were the severity of associated organ dysfunctions (OR, 1.20; 95% CI, 1.05 to 1.34), ARDS (OR, 2.31; 95% CI, 1.10 to 4.82) and positive fluid balance (OR, 2.09; 95% CI, 1.02 to 4.30).
Conclusions: Current mortality of ventilated patients in Brazil is elevated. Implementation of judicious fluid therapy and a watchful use and monitoring of NIV patients are potential targets to improve outcomes in this setting.
Trial registration: ClinicalTrials.gov NCT01268410.
Figures



Comment in
-
Lower tidal volumes in Brazil, also in patients without acute respiratory distress syndrome?Crit Care. 2013 Jun 12;17(3):436. doi: 10.1186/cc12721. Crit Care. 2013. PMID: 23767847 Free PMC article. No abstract available.
-
Authors’ response.Crit Care. 2013;17(3):436. Crit Care. 2013. PMID: 25207335 No abstract available.
References
-
- Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM. The epidemiology of mechanical ventilation use in the United States. Crit Care Med. 2010;38:1947–1953. - PubMed
-
- Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Villar J, Blanco J, Añón JM, Santos-Bouza A, Blanch L, Ambrós A, Gandía F, Carriedo D, Mosteiro F, Basaldúa S, Fernández RL, Kacmarek RM. ALIEN Network. The ALIEN study: incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Med. 2011;37:1932–1941. doi: 10.1007/s00134-011-2380-4. - DOI - PubMed
-
- Herridge MS, Tansey CM, Matté A, Tomlinson G, Diaz-Granados N, Cooper A, Guest CB, Mazer CD, Mehta S, Stewart TE, Kudlow P, Cook D, Slutsky AS, Cheung AM. Canadian Critical Care Trials Group. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364:1293–1304. doi: 10.1056/NEJMoa1011802. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
