

Chemokine (C-C motif) Ligand 2 is a potential biomarker of inflammation & physical fitness in obese children: a cross-sectional study
- PMID: 23557387
- PMCID: PMC3636051
- DOI: 10.1186/1471-2431-13-47
Chemokine (C-C motif) Ligand 2 is a potential biomarker of inflammation & physical fitness in obese children: a cross-sectional study
Abstract
Background: Obesity is a global epidemic that is impacting children around the world. Obesity is a chronic inflammatory state with enhanced production of multiple cytokines and chemokines. Chemokine (C-C motif) Ligand 2 (CCL2) is produced by immune and metabolic cells and attracts immune cells into liver, muscle and adipose tissue, resulting in initiation and propagation of the inflammatory response in obesity. How obesity and fitness affect the production of this chemokine in children is unknown.This study tested the hypotheses that CCL2 levels are higher in obese children when compared to lean controls, and that fitness modulates CCL2 levels allowing its use as a biomarker of fitness.
Methods: This was a cross sectional case-control study conducted in a Pediatric Tertiary care center in Hamilton, Ontario, Canada. Controls were recruited from the community. This study recruited overweight/obese children (BMI ≥ 85th percentile, n = 18, 9 female, mean age 14.0 ± 2.6 years) and lean controls (BMI < 85th percentile, n = 18, 8 female, mean age 14.0 ± 2.6 years) matched for age, sex and biological maturation.Aerobic fitness test was done using a cycle ergometer performing the McMaster All-Out Progressive Continuous Cycling test to exhaustion to determine peak oxygen uptake. Fasting CCL2 samples were taken prior to test. Categorical variables including subject categorization into different aerobic fitness levels in overweight/obese and lean children was reported based on the median split in each group.
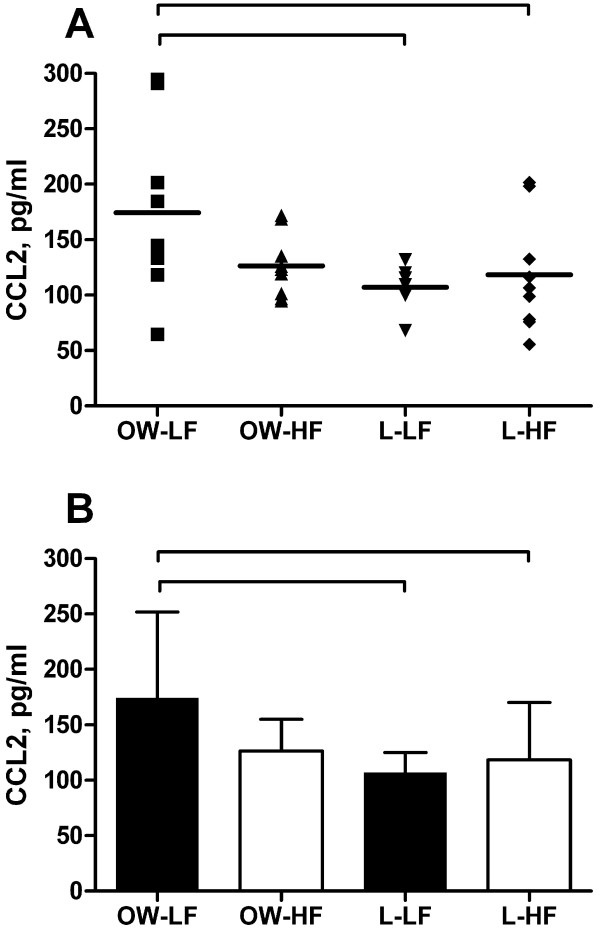
Results: Obese participants had significantly higher CCL2 levels when compared to lean group (150.4 ± 61.85 pg/ml versus 112.7 ± 38 pg/ml, p-value 0.034).To establish if CCL2 is a biomarker of fitness, we divided the groups based on their fitness levels. There was a main effect for group (F (3,32) = 3.2, p = 0.036). Obese high fitness group were similar to lean unfit and fit participants. Post-hoc analysis revealed that the overweight/obese low fitness group had significantly higher level of CCL2 compared to the lean low fitness group when adjusted to age, sex and maturity offset (F (3,29) = 3.1, p = 0.04).
Conclusions: CCL2 serves a dual role as a potential biomarker of inflammation and fitness in obese children.
Figures
References
-
- International Obesity Task Force. 2012. http://www.iaso.org; Accessed August 16th 2012.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
