

Reducing surgical site infections in hepatopancreatobiliary surgery
- PMID: 23557410
- PMCID: PMC3633041
- DOI: 10.1111/j.1477-2574.2012.00604.x
Reducing surgical site infections in hepatopancreatobiliary surgery
Abstract
Objectives: Patients undergoing complex hepatopancreatobiliary (HPB) operations are at high risk for surgical site infection (SSI). Factors such as biliary obstruction, operative time and pancreatic or biliary fistulae contribute to the high SSI rate. The purpose of this study was to analyse whether a multifactorial approach would reduce the incidence and cost of SSI after HPB surgery.
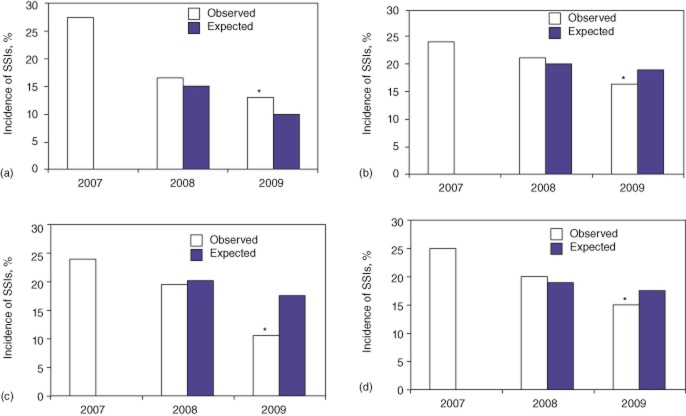
Methods: From January 2007 to December 2009, 895 complex HPB operations were monitored for SSI through the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP). In 2008, surgeon-specific SSI rates were provided to HPB surgeons, and guidelines for the management of perioperative factors were established. Observed SSI rates were monitored before and after these interventions. Hospital cost data were analysed and cost savings were calculated.
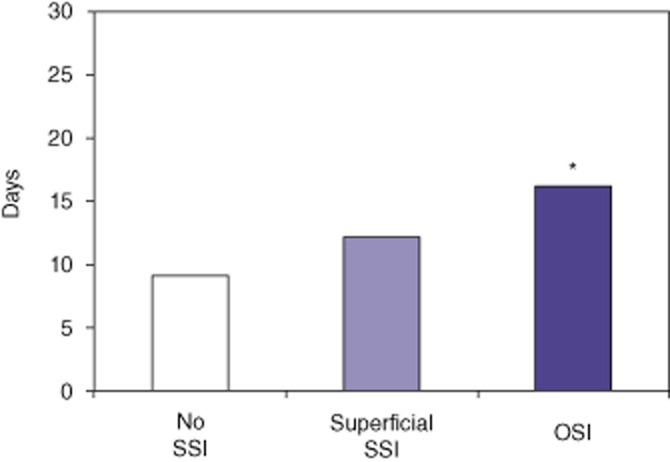
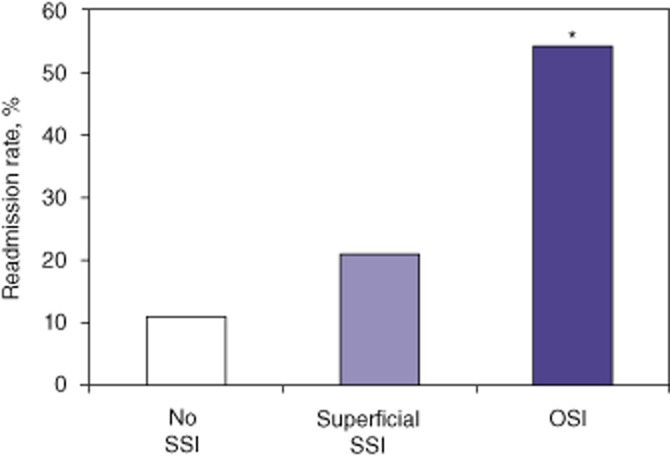
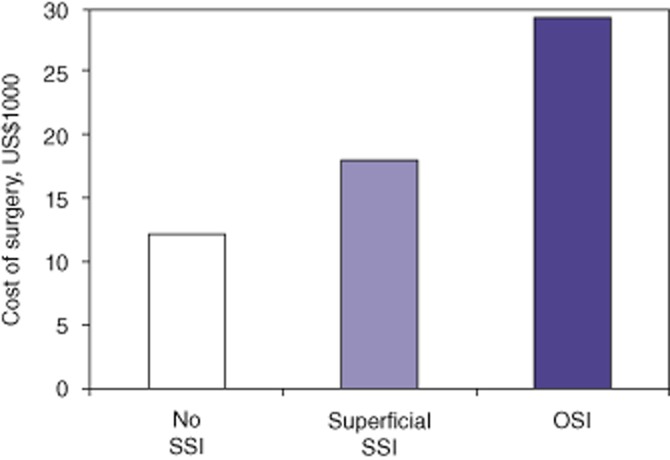
Results: Observed SSI for hepatic, pancreatic and complex biliary operations decreased by 9.6% over a 2-year period (P < 0.03). The excess cost per SSI was US$11 462 and was driven by increased length of stay and hospital readmission for infection. Surgeons rated surgeon-specific feedback on SSI rate as the most important factor in improvement.
Conclusions: High SSI rates following complex HPB operations can be improved by a multifactorial approach that features process improvements, individual surgeon feedback and reduced variation in patient management.
© 2012 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Andersson R, Saarela A, Tranberg KG, Bengmark S. Intra-abdominal abscess formation after major liver resection. Acta Chir Scand. 1990;156:707–710. - PubMed
-
- Kelly KJ, Greenblatt DY, Wan Y, Rettammel RJ, Winslow E, Cho CS, et al. Risk stratification for distal pancreatectomy utilizing ACS-NSQIP: preoperative factors predict morbidity and mortality. J Gastrointest Surg. 2011;15:250–259. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
