

Acute ST-elevation myocardial infarction in patients hospitalized for noncardiac conditions
- PMID: 23557748
- PMCID: PMC3647284
- DOI: 10.1161/JAHA.113.000004
Acute ST-elevation myocardial infarction in patients hospitalized for noncardiac conditions
Abstract
Background: Major advances have been made in the treatment of ST-elevation myocardial infarction (STEMI) in outpatients. In contrast, little is known about outcomes in STEMI that occur in patients hospitalized for a noncardiac condition.
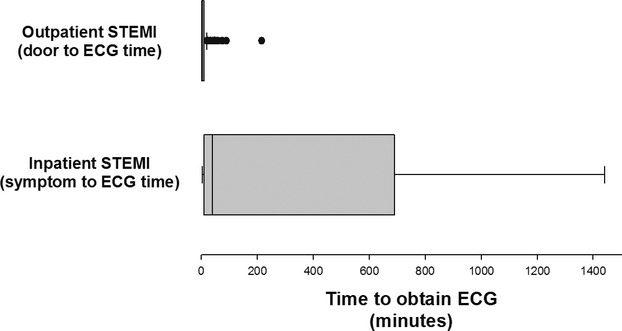
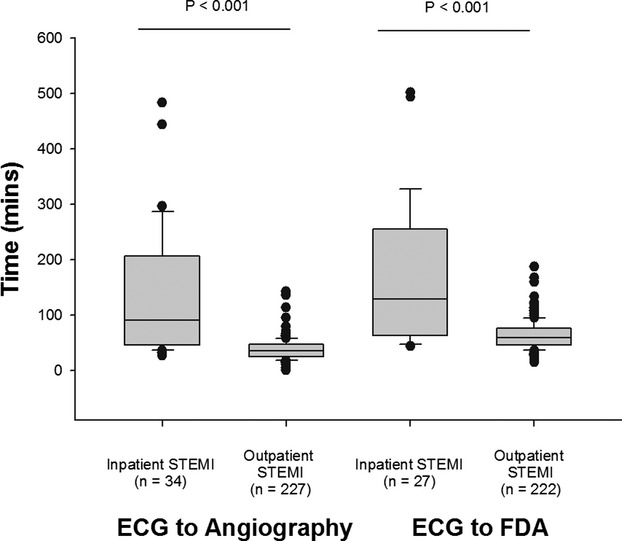
Methods and results: This was a retrospective, single-center study of inpatient STEMIs from January 1, 2007, to July 31, 2011. Forty-eight cases were confirmed to be inpatient STEMIs of a total of 139 410 adult discharges. These patients were older and more often female and had higher rates of chronic kidney disease and prior cerebrovascular events compared with 227 patients with outpatient STEMIs treated during the same period. Onset of inpatient STEMI was heralded most frequently by a change in clinical status (60%) and less commonly by patient complaints (33%) or changes on telemetry. Coronary angiography and percutaneous coronary intervention were performed in 71% and 56% of patients, respectively. The median time to obtain ECG (41 [10, 600] versus 5 [2, 10] minutes; P<0.001), ECG to angiography time (91 [26, 209] versus 35 [25, 46] minutes; P<0.001) and ECG to first device activation (FDA) (129 [65, 25] versus 60 [47, 76] minutes; P<0.001) were longer for inpatient versus outpatient STEMI. Survival to discharge was lower for inpatient STEMI (60% versus 96%; P<0.001), and this difference persisted after adjusting for potential confounders.
Conclusions: Patients who develop a STEMI while hospitalized for a noncardiac condition are older and more often female, have more comorbidities, have longer ECG-to-FDA times, and are less likely to survive than patients with an outpatient STEMI.
Figures
References
-
- Thygesen K, Alpert JS, White HDJoint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction Universal definition of myocardial infarction. J Am Coll Cardiol. 2007; 50:2173-2195 - PubMed
-
- Kushner FG, Hand M, Smith SC, Jr, King SB, III, Anderson JL, Antman EM, Bailey SR, Bates ER, Blankenship JC, Casey DE, Jr, Green LA, Hochman JS, Jacobs AK, Krumholz HM, Morrison DA, Ornato JP, Pearle DL, Peterson ED, Sloan MA, Whitlow PL, Williams DO. 2009 Focused updates: ACC/AHA guidelines for the management of patients with ST‐elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2009; 120:2271-2306 - PubMed
-
- Zymslinski RW, Lackland DT, Keil JE, Higgins JE. Increased fatality and difficult diagnosis of in‐hospital acute myocardial infarction: comparison to lower mortality and more easily recognized pre‐hospital infarction. Am Heart J. 1981; 101:586-592 - PubMed
-
- Zahn R, Schiele R, Seidl K, Kapp T, Glunz HG, Jagodzinski E, Voigtländer T, Gottwik M, Berg G, Thomas H, Senges J. Acute myocardial infarction occurring in versus out of the hospital: patient characteristics and clinical outcome. J Am Coll Cardiol. 2000; 35:1820-1826 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
