

Acute and chronic traumatic encephalopathies: pathogenesis and biomarkers
- PMID: 23558985
- PMCID: PMC4006940
- DOI: 10.1038/nrneurol.2013.36
Acute and chronic traumatic encephalopathies: pathogenesis and biomarkers
Abstract
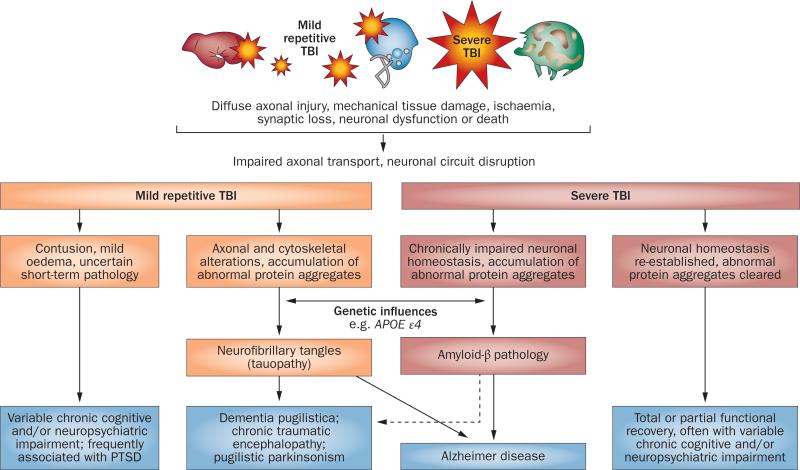
Over the past decade, public awareness of the long-term pathological consequences of traumatic brain injury (TBI) has increased. Such awareness has been stimulated mainly by reports of progressive neurological dysfunction in athletes exposed to repetitive concussions in high-impact sports such as boxing and American football, and by the rising number of TBIs in war veterans who are now more likely to survive explosive blasts owing to improved treatment. Moreover, the entity of chronic traumatic encephalopathy (CTE)--which is marked by prominent neuropsychiatric features including dementia, parkinsonism, depression, agitation, psychosis, and aggression--has become increasingly recognized as a potential late outcome of repetitive TBI. Annually, about 1% of the population in developed countries experiences a clinically relevant TBI. The goal of this Review is to provide an overview of the latest understanding of CTE pathophysiology, and to delineate the key issues that are challenging clinical and research communities, such as accurate quantification of the risk of CTE, and development of reliable biomarkers for single-incident TBI and CTE.
Figures
References
-
- Centers for Disease Control and Prevention . Injury prevention and control: traumatic brain injury. Centers for Disease Control and Prevention; 2012. [online], http://www.cdc.gov/traumaticbraininjury/statistics.html.
-
- DeKosky ST, Ikonomovic MD, Gandy S. Traumatic brain injury—football, warfare, and long-term effects. N. Engl. J. Med. 2010;363:1293–1296. - PubMed
-
- US Department of Defense . Traumatic brain injury—Department of Defense special report. US Department of Defense; 2012. [online], http://www.defense.gov/home/features/2012/0312_tbi/
-
- Lange RT, Brickell TA, Ivins B, Vanderploeg R, French LM. Variable, not always persistent, postconcussion symptoms following mild TBI in U.S. military service members: a 5-year cross-sectional outcome study. J. Neurotrauma. http://dx.doi.org/10.1089/neu.2012.2743. - DOI - PubMed
-
- Wall PL. Posttraumatic stress disorder and traumatic brain injury in current military populations: a critical analysis. J. Am. Psychiatr. Nurses Assoc. 2012;18:278–298. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
