

Case Reports
doi: 10.1681/ASN.2012070665.
Epub 2013 Apr 4.
AKI in an HIV patient
Affiliations
- PMID: 23559580
- PMCID: PMC3736712
- DOI: 10.1681/ASN.2012070665
Item in Clipboard
Case Reports
AKI in an HIV patient
J Am Soc Nephrol.
2013 Jul.
Abstract
The renal manifestations of patients infected with HIV are diverse. Patients may have podocytopathies ranging from a minimal-change-type lesions to FSGS or collapsing glomerulopathy. Furthermore, such patients produce a variety of autoantibodies without clinical signs of the disease. Antiretroviral drugs also cause renal injury, including crystals and tubular injury, acute interstitial nephritis, or mitochondrial toxicity. In these circumstances, it is essential to perform a renal biopsy for diagnosis and to guide treatment. Here we describe a patient with HIV who presented with AKI and hematuria without concomitant systemic manifestations. Renal biopsy elucidated the cause of acute deterioration of kidney function.
Figures
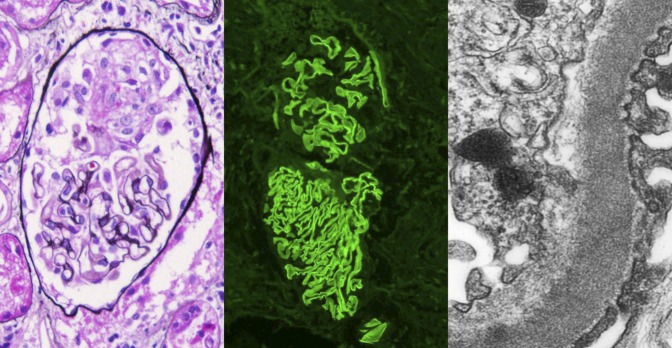
Crescentic GN with linear GBM staining on immunofluorescence. There is a small cellular crescent with fibrinoid material, with no proliferation or sclerosis of the glomerular tuft (left panel, Jones silver stain; original magnification ×400). By immunofluorescence, there is linear staining along the GBM with antibody to IgG. The top glomerulus also shows a small cellular crescent (middle panel, anti-IgG immunofluorescence; original magnification ×200). By electron microscopy, a high-power view of the capillary wall shows intact foot processes (right), and no deposits were present in a subepithelial or subendothelial location. Reticular aggregates were present in the endothelial cell cytoplasm, consistent with high interferon levels in this HIV-positive patient (transmission electron microscopy; original magnification ×8000).
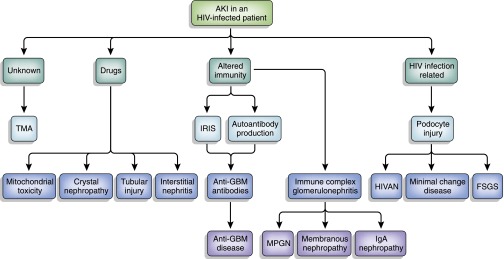
Schema of pathophysiologic mechanisms of AKI in HIV-positive patients. HIVAN, HIV-associated nephropathy; IRIS, immune reconstitution inflammatory syndrome; MNGN, membranoproliferative GN; TMA, thrombotic microangiopathy.
References
-
- Wearne N, Swanepoel CR, Boulle A, Duffield MS, Rayner BL: The spectrum of renal histologies seen in HIV with outcomes, prognostic indicators and clinical correlations. Nephrol Dial Transplant 27: 4109–4118, 2012 - PubMed
-
- Fine DM, Fogo AB, Alpers CE: Thrombotic microangiopathy and other glomerular disorders in the HIV-infected patient. Semin Nephrol 28: 545–555, 2008 - PubMed
-
- Monteiro EJB, Caron D, Balda CA, Franco M, Pereira AB, Kirsztajn GM: Anti-glomerular basement membrane glomerulonephritis in an HIV positive patient: Case report. Braz J Infect Dis 10: 55–58, 2006 - PubMed
-
- Wechsler E, Yang T, Jordan SC, Vo A, Nast CC: Anti-glomerular basement membrane disease in an HIV-infected patient. Nat Clin Pract Nephrol 4: 167–171, 2008 - PubMed
-
- Singh P, Barry M, Tzamaloukas A: Goodpasture’s disease complicating human immunodeficiency virus infection. Clin Nephrol 76: 74–77, 2011 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
