

Results of surgical excision of cirsoid aneurysm of the scalp without preoperative interventions
- PMID: 23559986
- PMCID: PMC3613641
- DOI: 10.4103/1793-5482.106651
Results of surgical excision of cirsoid aneurysm of the scalp without preoperative interventions
Abstract
Context: Cirsoid aneurysms of scalp are rare lesions which are mainly treated by surgical excision. Endovascular embolization was described either alone or prior to surgery in order to minimize the risk of bleeding. However, the endovascular therapy also carries the risk of scalp necrosis, escape of embolization material to circulation, and recurrence of the lesion.
Aim: To evaluate the results of well-planned classic surgical excision of cirsoid aneurysm.
Study design: This is a retrospective case series study.
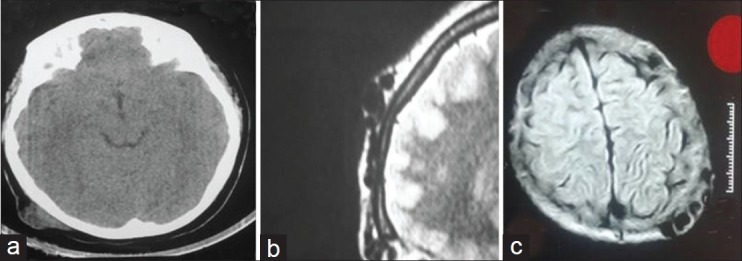
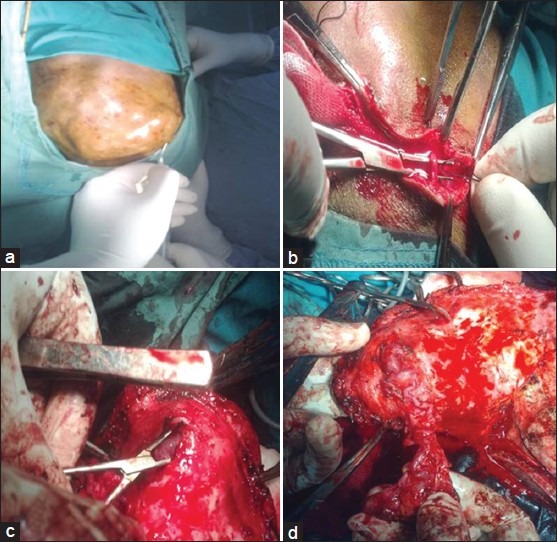
Materials and methods: This is a retrospective case series study on nine patients with cirsoid aneurysms who were treated with surgical excision. Preoperative Planning for location, size, feeding arteries, and venous drainage of the lesions were done by plain and contrast enhanced CT, MRI, MR angiogram, and selective internal and external carotid angiograms. Complete surgical excision for the lesions was done. Postoperative evaluation of excision was done by cranial magnetic resonance angiography in all the patients. The mean follow up period was 34.1 (±7.62 STD) months.
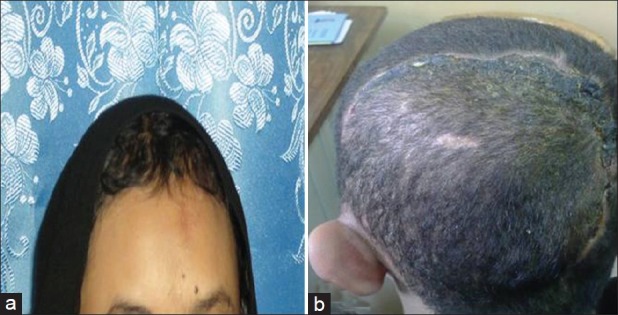
Results: The lesion was located in the occipital region in three (33.3%) cases, frontal region in two (22.2%) cases, temproparietal region in two (22.2%) cases, parietal region in one case (11.1%), and vertex in one case (11.1%). The superficial temporal artery was involved in seven (77.8%) cases, the occipital artery was involved in six (66.7%) cases, the posterior auricular artery was involved in five (55.6%) cases, the supraorbital artery was involved in two (22.2%) cases and the middle meningeal artery was involved in two (22.2%) cases. Total excision of the lesion was achieved in eight patients and en bloc resection and primary closure was done in one patient. Postoperative magnetic resonance angiogram showed no residual lesion in all patients. No postoperative complication related to the surgery had occurred. No recurrence had occurred during the follow-up period (mean 34.1 ± 7.62 STD months).
Conclusion: Well-planned surgery of cirsoid aneurysm of the scalp without preoperative interventions could achieve complete excision of the lesion without any residual masses or recurrence and with a low incidence of complications.
Keywords: Arteriovenous fistula; cirsoid aneurysm; scalp; vascular malformation.
Conflict of interest statement
Figures



References
-
- Muthukumar N, Rajagopal V, Manoharan AV, Durairaj N. Surgical Management of Cirsoid Aneurysms. ActaNeurochir. 2002;144:349–56. - PubMed
-
- Barnwell SL, Halbach VV, Dowd CF, Higshida RT, Hieshima GB. Endovascular treatment of scalp arteriovenous fistulas associated with a large varix. Radiology. 1989;173:533–9. - PubMed
-
- Gurkanlar D, Gonul M, Solmaz I, Gonul E. Cirsoid aneurysms of the scalp. Neurosurg Rev. 2006;29:208–12. - PubMed
-
- Fisher-Jeffes ND, Domingo Z, Madden M, De Villiers JC. Arteriovenous malformations of the scalp. Neurosurgery. 1995;36:656–60. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials