

The prospective, observational, multicenter, major trauma transfusion (PROMMTT) study: comparative effectiveness of a time-varying treatment with competing risks
- PMID: 23560283
- PMCID: PMC3740072
- DOI: 10.1001/2013.jamasurg.387
The prospective, observational, multicenter, major trauma transfusion (PROMMTT) study: comparative effectiveness of a time-varying treatment with competing risks
Abstract
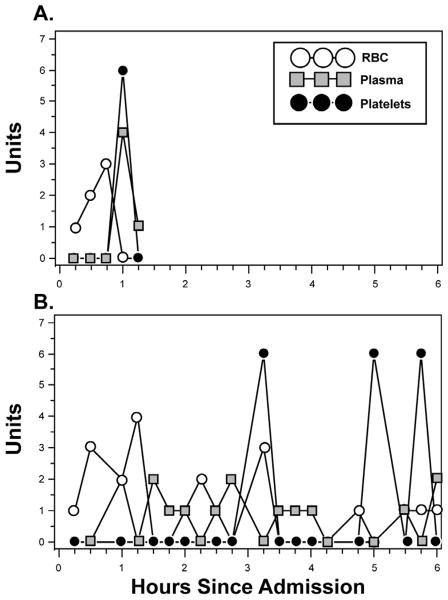
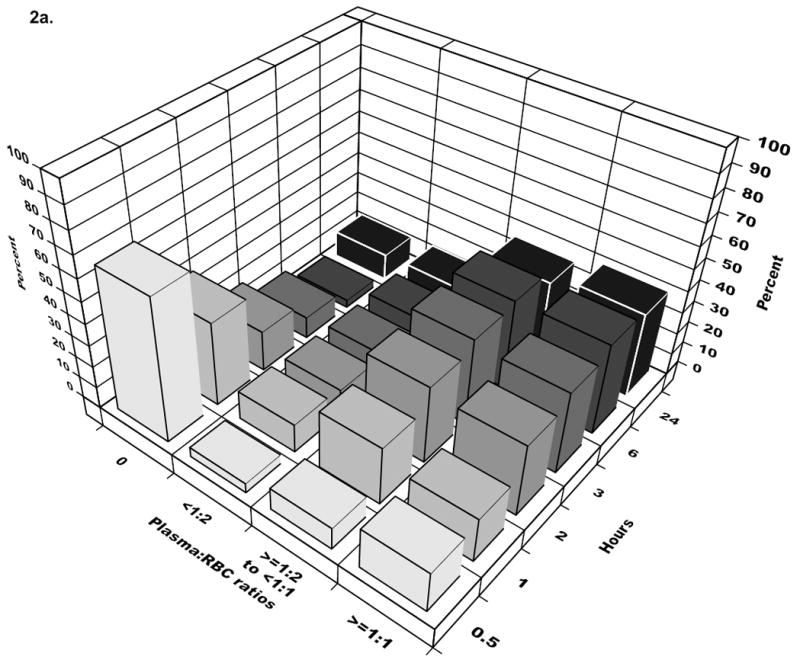
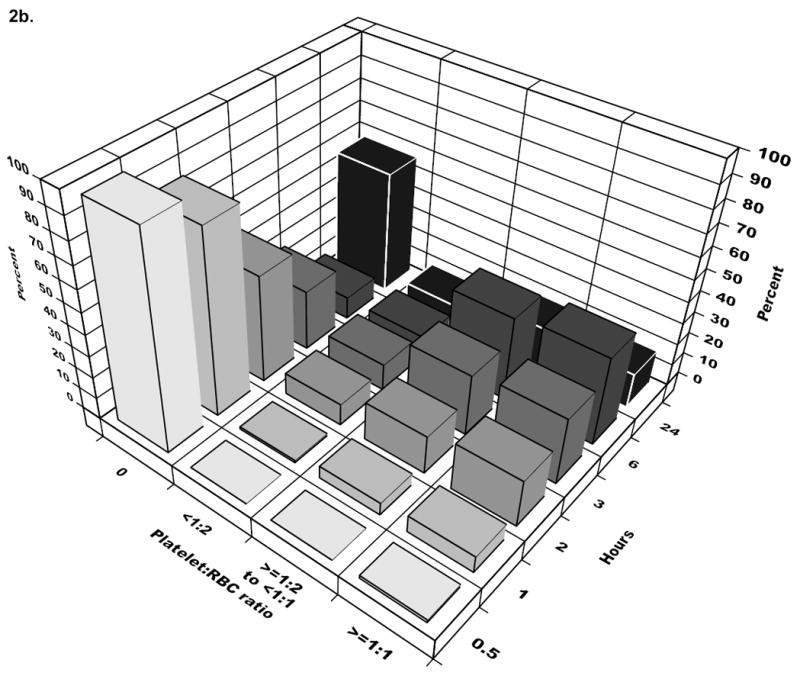
Objective: To relate in-hospital mortality to early transfusion of plasma and/or platelets and to time-varying plasma:red blood cell (RBC) and platelet:RBC ratios.
Design: Prospective cohort study documenting the timing of transfusions during active resuscitation and patient outcomes. Data were analyzed using time-dependent proportional hazards models.
Setting: Ten US level I trauma centers.
Patients: Adult trauma patients surviving for 30 minutes after admission who received a transfusion of at least 1 unit of RBCs within 6 hours of admission (n = 1245, the original study group) and at least 3 total units (of RBCs, plasma, or platelets) within 24 hours (n = 905, the analysis group).
Main outcome measure: In-hospital mortality.
Results: Plasma:RBC and platelet:RBC ratios were not constant during the first 24 hours (P < .001 for both). In a multivariable time-dependent Cox model, increased ratios of plasma:RBCs (adjusted hazard ratio = 0.31; 95% CI, 0.16-0.58) and platelets:RBCs (adjusted hazard ratio = 0.55; 95% CI, 0.31-0.98) were independently associated with decreased 6-hour mortality, when hemorrhagic death predominated. In the first 6 hours, patients with ratios less than 1:2 were 3 to 4 times more likely to die than patients with ratios of 1:1 or higher. After 24 hours, plasma and platelet ratios were unassociated with mortality, when competing risks from nonhemorrhagic causes prevailed.
Conclusions: Higher plasma and platelet ratios early in resuscitation were associated with decreased mortality in patients who received transfusions of at least 3 units of blood products during the first 24 hours after admission. Among survivors at 24 hours, the subsequent risk of death by day 30 was not associated with plasma or platelet ratios.
Conflict of interest statement
Figures
Comment in
-
Resuscitation strategies in trauma.JAMA. 2013 Jun 5;309(21):2270-1. doi: 10.1001/jama.2013.5161. JAMA. 2013. PMID: 23736736 No abstract available.
-
CAGS and ACS evidence based reviews in surgery. 50. Is early transfusion of plasma and platelets in higher ratios associated with decreased in-hospital mortality in bleeding patients?Can J Surg. 2014 Oct;57(5):358-60. doi: 10.1503/cjs.010314. Can J Surg. 2014. PMID: 25265113 Free PMC article. No abstract available.
References
-
- Lopez AD, Mathers CD. Measuring the global burden of disease and epidemiological transitions: 2002–2030. Ann Trop Med Parasitol. 2006;100(5–6):481–499. - PubMed
-
- Sleet DA, Moffett DB. Framing the problem: injuries and public health. Fam Community Health. 2009;32(2):88–97. - PubMed
-
- Eastman AB. Wherever the dart lands: toward the ideal trauma system. J Am Coll Surg. 2010;211(2):153–168. - PubMed
-
- Hoyt DB. Blood and war-lest we forget. J Am Coll Surg. 2009;209(6):681–686. - PubMed
-
- Evans JA, van Wessem KJ, McDougall D, Lee KA, Lyons T, Balogh ZJ. Epidemiology of traumatic deaths: comprehensive population-based assessment. World J Surg. 2010;34(1):158–163. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
