

Mortality predictability of body size and muscle mass surrogates in Asian vs white and African American hemodialysis patients
- PMID: 23562348
- PMCID: PMC3909735
- DOI: 10.1016/j.mayocp.2013.01.025
Mortality predictability of body size and muscle mass surrogates in Asian vs white and African American hemodialysis patients
Abstract
Objective: To determine whether the association of body size and muscle mass with survival among patients undergoing long-term hemodialysis (HD) is consistent across race, especially in East Asian vs white and African American patients.
Patients and methods: Using data from 20,818 patients from South Korea who underwent HD from February 1, 2001, to June 30, 2009, and 20,000 matched patients from the United States (10,000 whites and 10,000 African Americans) who underwent HD from July 1, 2001, to June 30, 2006, we compared mortality associations of baseline body mass index (BMI) and serum creatinine level as likely surrogates of obesity and muscle mass across the 3 races.
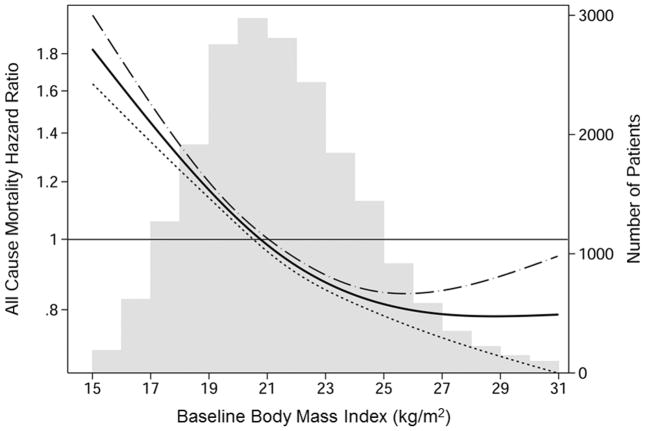
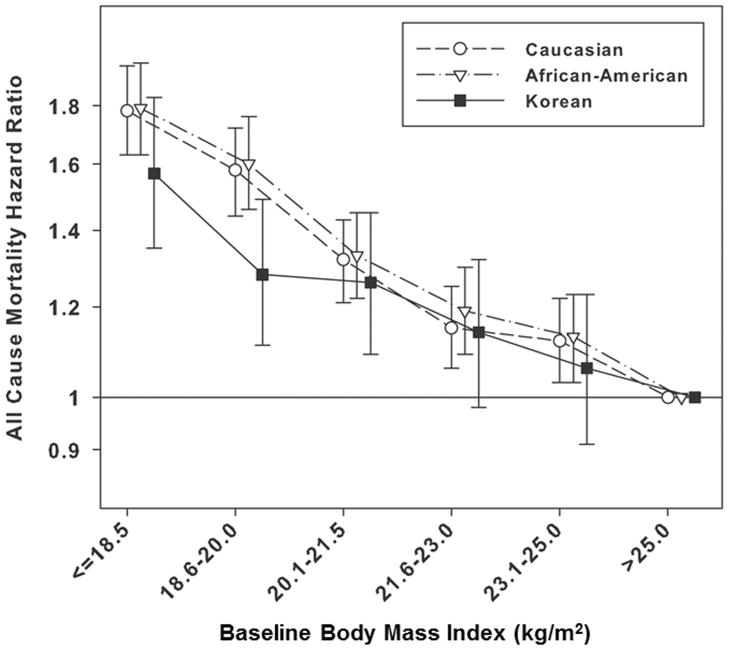
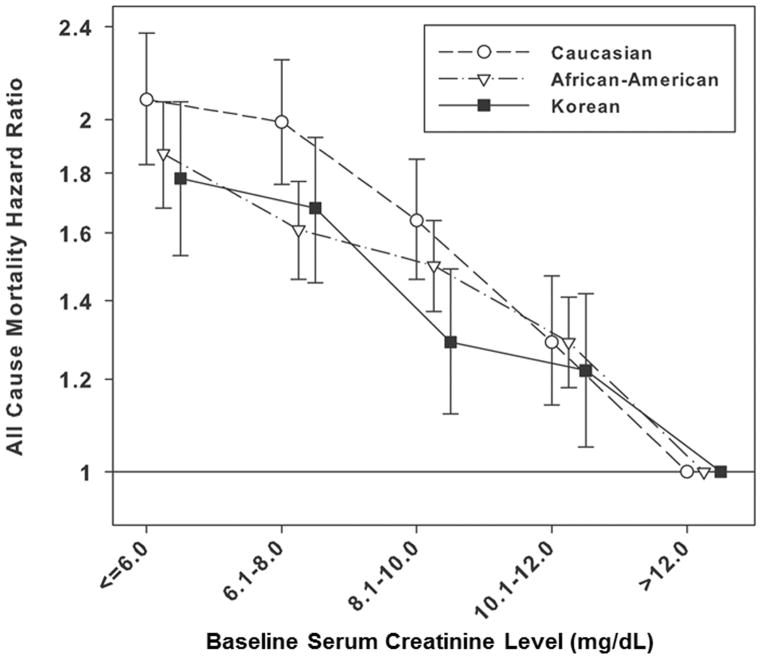
Results: In Korean HD patients, higher BMI together with higher serum creatinine levels were associated with greater survival, as previously reported from US and European studies. In the matched cohort (10,000 patients from each of the 3 races), mortality risks were lower across higher BMI and serum creatinine levels, and these associations were similar in all 3 races (reference groups: patients with BMI >25.0 kg/m(2) or serum creatinine >12 mg/dL in each race). White, African American, and Korean patients with BMI levels of 18.5 kg/m(2) or less (underweight) had 78%, 79%, and 57% higher mortality risk, respectively, and white, African American, and Korean patients with serum creatinine levels of 6.0 mg/dL or less had 108%, 87%, and 78% higher mortality, respectively.
Conclusion: This study shows that race does not modify the association of higher body size and muscle mass with greater survival in HD patients. Given the consistency of the obesity paradox, which may be related to a mitigated effect of protein-energy wasting on mortality irrespective of racial disparities, nutritional support to improve survival should be tested in HD patients of all races.
Copyright © 2013 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- USRDS. [Accessed April 10, 2012];Annual Data Report: Atlas of End-Stage Renal Disease in the United States. 2011 http://www.usrds.org/atlas.asps. - PubMed
-
- Chertow GM, Hsu CY, Johansen KL. The enlarging body of evidence: obesity and chronic kidney disease. J Am Soc Nephrol. 2006 Jun;17(6):1501–1502. - PubMed
-
- Kovesdy CP, Anderson JE, Kalantar-Zadeh K. Paradoxical association between body mass index and mortality in men with CKD not yet on dialysis. Am J Kidney Dis. 2007 May;49(5):581–591. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
