

Direct or coincidental elimination of stable rotors or focal sources may explain successful atrial fibrillation ablation: on-treatment analysis of the CONFIRM trial (Conventional ablation for AF with or without focal impulse and rotor modulation)
- PMID: 23563126
- PMCID: PMC3703494
- DOI: 10.1016/j.jacc.2013.03.021
Direct or coincidental elimination of stable rotors or focal sources may explain successful atrial fibrillation ablation: on-treatment analysis of the CONFIRM trial (Conventional ablation for AF with or without focal impulse and rotor modulation)
Abstract
Objectives: This study sought to determine whether ablation of recently described stable atrial fibrillation (AF) sources, either directly by Focal Impulse and Rotor Modulation (FIRM) or coincidentally when anatomic ablation passes through AF sources, may explain long-term freedom from AF.
Background: It is unclear why conventional anatomic AF ablation can be effective in some patients yet ineffective in others with similar profiles.
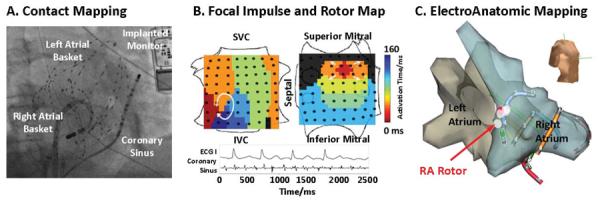
Methods: The CONFIRM (Conventional Ablation for AF With or Without Focal Impulse and Rotor Modulation) trial prospectively revealed stable AF rotors or focal sources in 98 of 101 subjects with AF at 107 consecutive ablation cases. In 1:2 fashion, subjects received targeted source ablation (FIRM) followed by conventional ablation, or conventional ablation alone. We determined whether ablation lesions on electroanatomic maps passed through AF sources on FIRM maps.
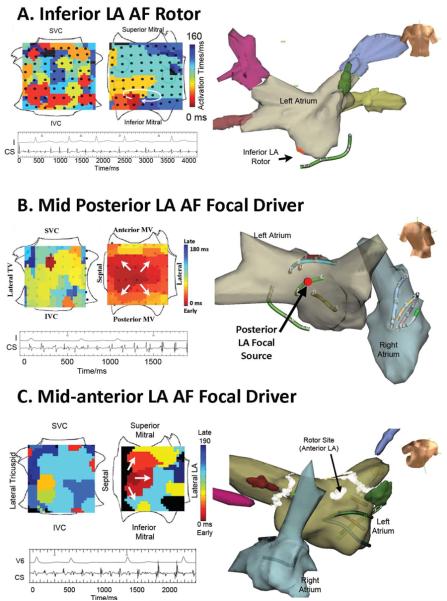
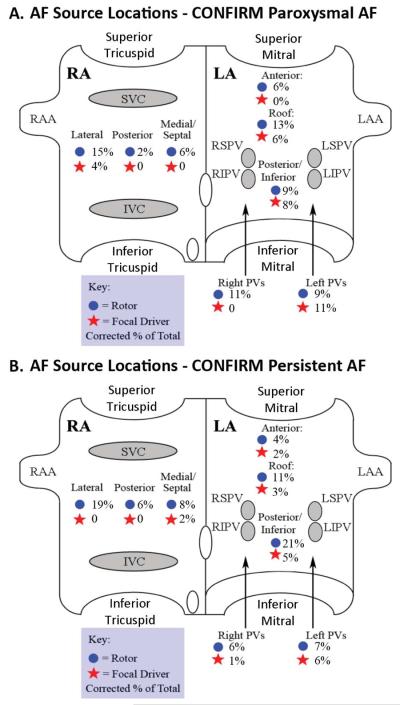
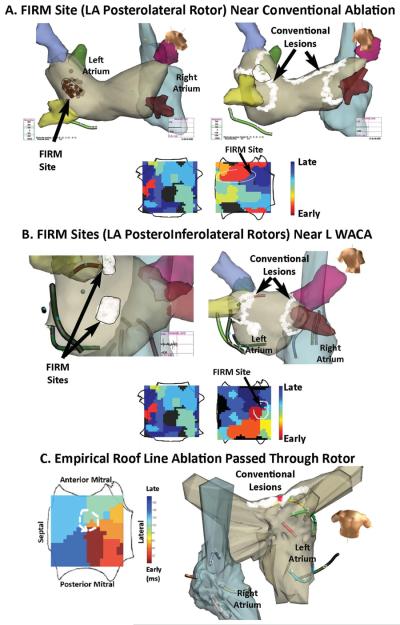
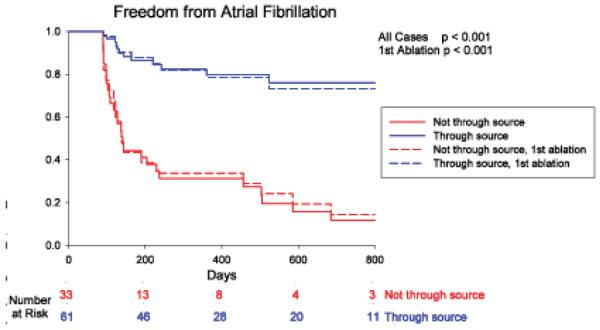
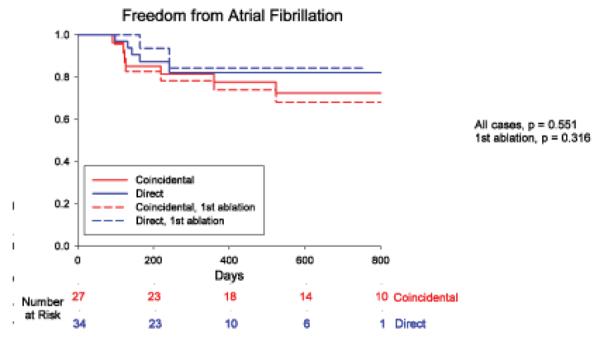
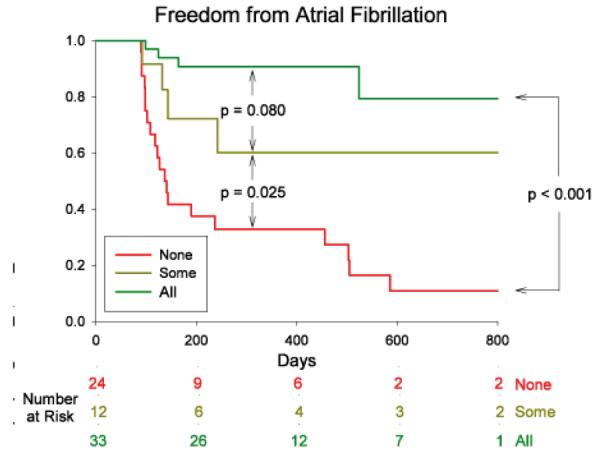
Results: Subjects who completed follow-up (n = 94; 71.2% with persistent AF) showed 2.3 ± 1.1 concurrent AF rotors or focal sources that lay near pulmonary veins (22.8%), left atrial roof (16.0%), and elsewhere in the left (28.2%) and right (33.0%) atria. AF sources were ablated directly in 100% of FIRM cases and coincidentally (e.g., left atrial roof) in 45% of conventional cases (p < 0.05). During a median (interquartile range) of 273 days (138 to 636 days) after one procedure, AF was absent in 80.3% of patients if sources were ablated but in only 18.2% of patients if sources were missed (p < 0.001). Freedom from AF was highest if all sources were ablated, intermediate if some sources were ablated, and lowest if no sources were ablated (p < 0.001).
Conclusions: Elimination of stable AF rotors and focal sources may explain freedom from AF after diverse approaches to ablation. Patient-specific AF source distributions are consistent with the reported success of specific anatomic lesion sets and of widespread ablation. These results support targeting AF sources to reduce unnecessary ablation, and motivate studies on FIRM-only ablation.
Trial registration: ClinicalTrials.gov NCT01008722.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Rotor ablation: around and around we go.J Am Coll Cardiol. 2013 Jul 9;62(2):148-149. doi: 10.1016/j.jacc.2013.04.035. Epub 2013 May 9. J Am Coll Cardiol. 2013. PMID: 23665096 No abstract available.
References
-
- Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362:1363–73. - PubMed
-
- Roy D, Talajic M, Nattel S, et al. Rhythm control versus rate control for atrial fibrillation and heart failure. N Engl J Med. 2008;358:2667–77. - PubMed
-
- Oral H, Pappone C, Chugh A, et al. Circumferential Pulmonary-Vein Ablation for Chronic Atrial Fibrillation. N Engl J Med. 2006;354:934–941. - PubMed
-
- Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010;303:333–40. - PubMed
-
- Morillo C, Verma A, Kuck KH, et al. Radiofrequency Ablation Vs Antiarrhythmic Drugs As First-lne Treatment Of Symptomatic Atrial Fibrillation: (RAAFT 2): A Randomized Trial (Late Breaking Abstract) Heart Rhythm. 2012;9 - PubMed
