

Hepatic dysfunction in ambulatory patients with heart failure: application of the MELD scoring system for outcome prediction
- PMID: 23563127
- PMCID: PMC3939720
- DOI: 10.1016/j.jacc.2012.12.056
Hepatic dysfunction in ambulatory patients with heart failure: application of the MELD scoring system for outcome prediction
Abstract
Objectives: This study evaluated the Model for End-Stage Liver Disease (MELD) score and its modified versions, which are established measures of liver dysfunction, as a tool to assess heart transplantation (HTx) urgency in ambulatory patients with heart failure.
Background: Liver abnormalities have a prognostic impact on the outcome of patients with advanced heart failure.
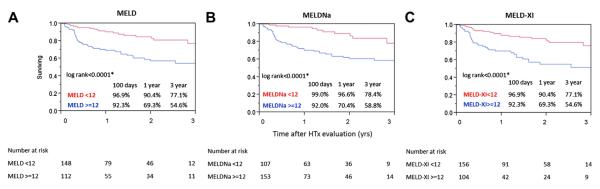
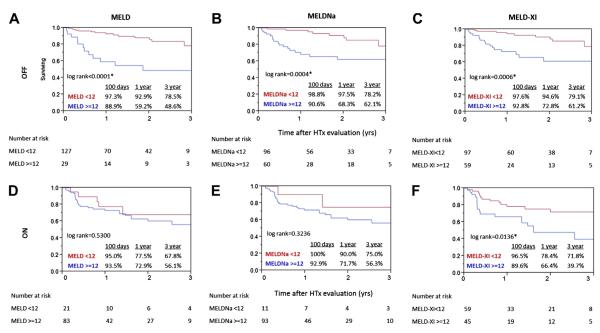
Methods: We retrospectively evaluated 343 patients undergoing HTx evaluation between 2005 and 2009. The prognostic effectiveness of MELD and 2 modifications (MELDNa [includes serum sodium levels] and MELD-XI [does not include international normalized ratio]) for endpoint events, defined as death/HTx/ventricular assist device requirement, was evaluated in our cohort and in subgroups of patients on and off oral anticoagulation.
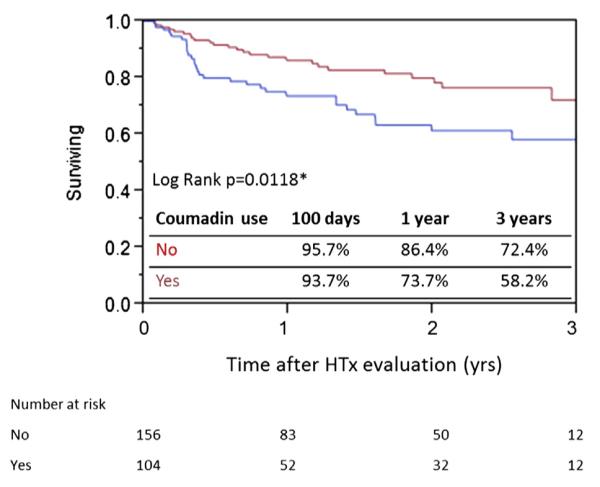
Results: The MELD and MELDNa scores were excellent predictors for 1-year endpoint events (areas under the curve: 0.71 and 0.73, respectively). High scores (>12) were strongly associated with poor survival at 1 year (MELD 69.3% vs. 90.4% [p < 0.0001]; MELDNa 70.4% vs. 96.9% [p < 0.0001]). Increased scores were associated with increased risk for HTx (hazard ratio: 1.10 [95% confidence interval: 1.06 to 1.14]; p < 0.0001 for both scores), which was independent of other known risk factors (MELD p = 0.0055; MELDNa p = 0.0083). Anticoagulant use was associated with poor survival at 1 year (73.7% vs. 86.4%; p = 0.0118), and the statistical significance of MELD/MELDNa was higher in patients not receiving oral anticoagulation therapy. MELD-XI was a fair but limited predictor of the endpoint events in patients receiving oral anticoagulation therapy.
Conclusions: Assessment of liver dysfunction according to the MELD scoring system provides additional risk information in ambulatory patients with heart failure.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The MELD scoring system and the prediction of outcomes in heart failure patients: what we have learned from the hepatologists.J Am Coll Cardiol. 2013 Jun 4;61(22):2262-3. doi: 10.1016/j.jacc.2013.02.064. Epub 2013 Apr 2. J Am Coll Cardiol. 2013. PMID: 23562922 No abstract available.
-
Cardiac hepatopathy versus end-stage liver disease: two different entities.J Am Coll Cardiol. 2014 May 6;63(17):1809-10. doi: 10.1016/j.jacc.2013.08.1654. Epub 2013 Dec 4. J Am Coll Cardiol. 2014. PMID: 24315902 No abstract available.
-
Reply: cardiac hepatopathy versus end-stage liver disease: two different entities.J Am Coll Cardiol. 2014 May 6;63(17):1810-1. doi: 10.1016/j.jacc.2013.10.065. Epub 2013 Dec 4. J Am Coll Cardiol. 2014. PMID: 24315904 No abstract available.
References
-
- Mancini DM, Eisen H, Kussmanul W, Mull R, Edmunds LH, Wilson JR. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation. 1991;83:778–86. - PubMed
-
- Aaronson KD, Schwartz JS, Chen TM, Wong KL, Goin JE, Mancini DM. Development and prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation. Circulation. 1997;95:2660–7. - PubMed
-
- Levy WC, Mozaffarian D, Linker DT, et al. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006;113:1424–33. - PubMed
-
- van Deursen VM, Damman K, Hillege HL, et al. Abnormal liver function in relation to hemodynamic profile in heart failure patients. J Card Fail. 2010;16:84–90. - PubMed
-
- Poelzl G, Ess M, Mussner-Seeber C, Pachinger O, Frick M, Ulmer H. Liver dysfunction in chronic heart failure: prevalence, characteristic and prognostic significance. Eur J Clin Invest. 2012;42:153–63. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical