

A comparison of two delivery modalities of a mobile phone-based assessment for serious mental illness: native smartphone application vs text-messaging only implementations
- PMID: 23563184
- PMCID: PMC3636800
- DOI: 10.2196/jmir.2328
A comparison of two delivery modalities of a mobile phone-based assessment for serious mental illness: native smartphone application vs text-messaging only implementations
Abstract
Background: Mobile phone-based assessment may represent a cost-effective and clinically effective method of monitoring psychotic symptoms in real-time. There are several software options, including the use of native smartphone applications and text messages (short message service, SMS). Little is known about the strengths and limitations of these two approaches in monitoring symptoms in individuals with serious mental illness.
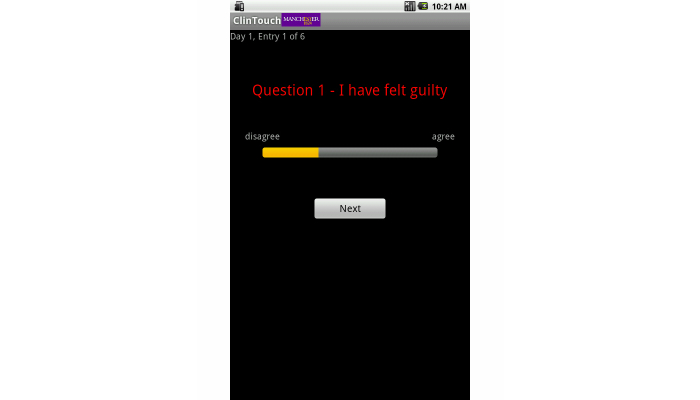
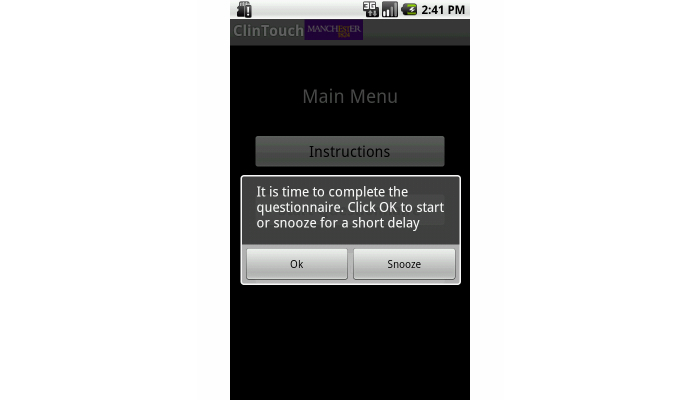
Objective: The objective of this study was to compare two different delivery modalities of the same diagnostic assessment for individuals with non-affective psychosis-a native smartphone application employing a graphical, touch user interface against an SMS text-only implementation. The overall hypothesis of the study was that patient participants with sewrious mental illness would find both delivery modalities feasible and acceptable to use, measured by the quantitative post-assessment feedback questionnaire scores, the number of data points completed, and the time taken to complete the assessment. It was also predicted that a native smartphone application would (1) yield a greater number of data points, (2) take less time, and (3) be more positively appraised by patient participant users than the text-based system.
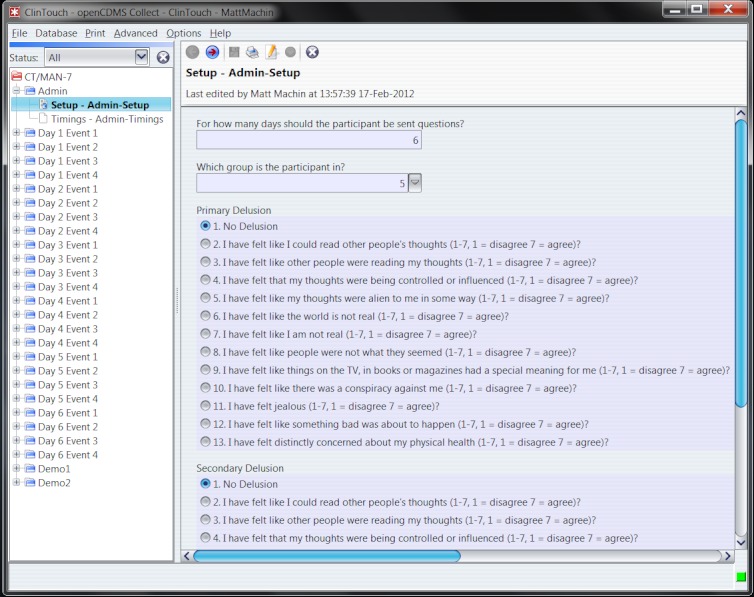
Methods: A randomized repeated measures crossover design was employed. Participants with currently treated Diagnostic and Statistical Manual (Fourth Edition) schizophrenia or related disorders (n=24) were randomly allocated to completing 6 days of assessment (four sets of questions per day) with a native smartphone application or the SMS text-only implementation. There was then a 1-week break before completing a further 6 days with the alternative delivery modality. Quantitative feedback questionnaires were administered at the end of each period of sampling.
Results: A greater proportion of data points were completed with the native smartphone application in comparison to the SMS text-only implementation (β = -.25, SE=.11, P=.02), which also took significantly less time to complete (β =.78, SE= .09, P<.001). Although there were no significant differences in participants' quantitative feedback for the two delivery modalities, most participants reported preferring the native smartphone application (67%; n=16) and found it easier to use (71%; n=16). 33% of participants reported that they would be willing to complete mobile phone assessment for 5 weeks or longer.
Conclusions: Native smartphone applications and SMS text are both valuable methods of delivering real-time assessment in individuals with schizophrenia. However, a more streamlined graphical user interface may lead to better compliance and shorter entry times. Further research is needed to test the efficacy of this technology within clinical services, to assess validity over longer periods of time and when delivered on patients' own phones.
Conflict of interest statement
Conflicts of Interest: Lewis has received speakers’ honoraria from the pharmaceutical companies AstraZeneca and Janssen. Shitij Kapur has had grant support from the pharmaceutical industry. Emma Barkus has received funding from P1vital a Precompetitive Consortium. There are no other declarations of interest. Shitij Kapur received partial salary support via the National Institute of Health Research Biomedical Research Centre at the South London and Maudsley NHSFT. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health
Figures
References
-
- Mangalore R, Knapp M. Cost of schizophrenia in England. J Ment Health Policy Econ. 2007 Mar;10(1):23–41. - PubMed
-
- Department of Health No health without mental health: A cross-government mental health outcomes strategy for people of all ages - supporting document. 2011. [2013-03-06]. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicati....
-
- Csikszentmihalyi M, Larson R. Validity and reliability of the Experience-Sampling Method. J Nerv Ment Dis. 1987 Sep;175(9):526–36. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
