

Cost-effectiveness and quality of life in surgeon versus general practitioner-organised colon cancer surveillance: a randomised controlled trial
- PMID: 23564936
- PMCID: PMC3641467
- DOI: 10.1136/bmjopen-2012-002391
Cost-effectiveness and quality of life in surgeon versus general practitioner-organised colon cancer surveillance: a randomised controlled trial
Abstract
Objective: To assess whether colon cancer follow-up can be organised by general practitioners (GPs) without a decline in the patient's quality of life (QoL) and increase in cost or time to cancer diagnoses, compared to hospital follow-up.
Design: Randomised controlled trial.
Setting: Northern Norway Health Authority Trust, 4 trusts, 11 hospitals and 88 local communities.
Participants: Patients surgically treated for colon cancer, hospital surgeons and community GPs.
Intervention: 24-month follow-up according to national guidelines at the community GP office. To ensure a high follow-up guideline adherence, a decision support tool for patients and GPs were used.
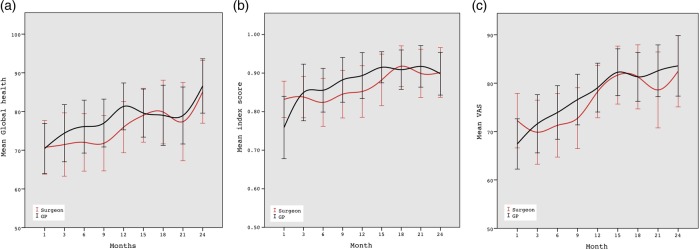
Main outcome measures: Primary outcomes were QoL, measured by the global health scales of the European Organisation for Research and Treatment of Cancer QoL Questionnaire (EORTC QLQ C-30) and EuroQol-5D (EQ-5D). Secondary outcomes were cost-effectiveness and time to cancer diagnoses.
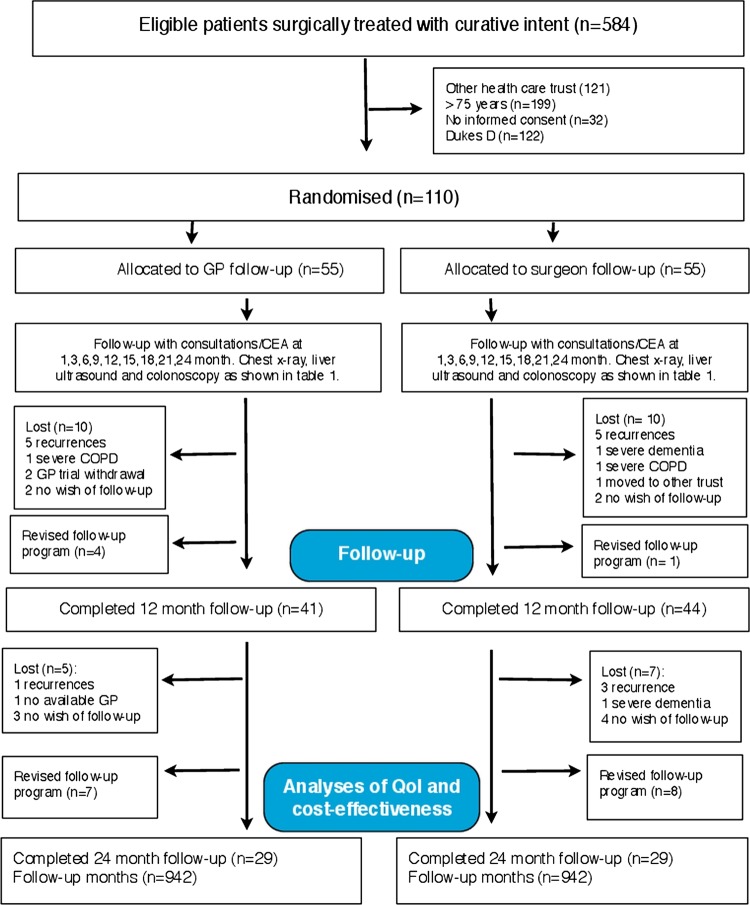
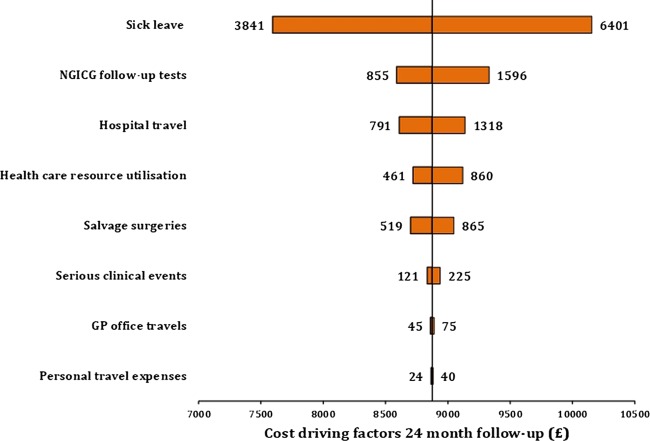
Results: 110 patients were randomised to intervention (n=55) or control (n=55), and followed by 78 GPs (942 follow-up months) and 70 surgeons (942 follow-up months), respectively. Compared to baseline, there was a significant improvement in postoperative QoL (p=0.003), but no differences between groups were revealed (mean difference at 1, 3, 6, 9, 12, 15, 18, 21 and 24-month follow-up appointments): Global Health; Δ-2.23, p=0.20; EQ-5D index; Δ-0.10, p=0.48, EQ-5D VAS; Δ-1.1, p=0.44. There were no differences in time to recurrent cancer diagnosis (GP 35 days vs surgeon 45 days, p=0.46); 14 recurrences were detected (GP 6 vs surgeon 8) and 7 metastases surgeries performed (GP 3 vs surgeon 4). The follow-up programme initiated 1186 healthcare contacts (GP 678 vs surgeon 508), 1105 diagnostic tests (GP 592 vs surgeon 513) and 778 hospital travels (GP 250 vs surgeon 528). GP organised follow-up was associated with societal cost savings (£8233 vs £9889, p<0.001).
Conclusions: GP-organised follow-up was associated with no decline in QoL, no increase in time to recurrent cancer diagnosis and cost savings.
Trial registration: ClinicalTrials.gov identifier NCT00572143.
Figures

References
-
- Larsen IK. Cancer in Norway 2009. Oslo, Norway: Cancer Registry of Norway, 2011:1–169
-
- Jeffery M, Hickey BE, Hider PN. Follow-up strategies for patients treated for non-metastatic colorectal cancer. Cochrane Database Syst Rev 2007; doi:10.1002/14651858.CD002200.pub2 - PubMed
-
- Tjandra JJ, Chan MKY. Follow-up after curative resection of colorectal cancer: a meta-analysis. Dis Colon Rectum 2007;50:1783–99 - PubMed
-
- Cairns SR, Scholefield JH, Steele RJ, et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk groups (update from 2002). Gut 2010;59:666e690. doi:10.1136/gut.2009. 179804 - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical