

Transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombus: a meta-analysis
- PMID: 23566041
- PMCID: PMC3626696
- DOI: 10.1186/1471-230X-13-60
Transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombus: a meta-analysis
Abstract
Background: Although transarterial chemoembolization (TACE) has been used extensively for advanced hepatocellular carcinoma (HCC) with portal vein tumor thrombus (PVTT), no consensus has been reached and an evidence base for practice is lacking. This meta-analysis evaluated the efficacy and safety of TACE for treatment of HCC with PVTT.
Methods: Ovid Medline, EMBASE, Web of Knowledge, and Cochrane library databases were searched up to August 2012 for controlled trials assessing TACE in patients with PVTT. Data concerning the study design, characteristics of trials, and outcomes were extracted. Hazard ratio (HR) and 95% confidence interval (CI) were calculated using random effects models.
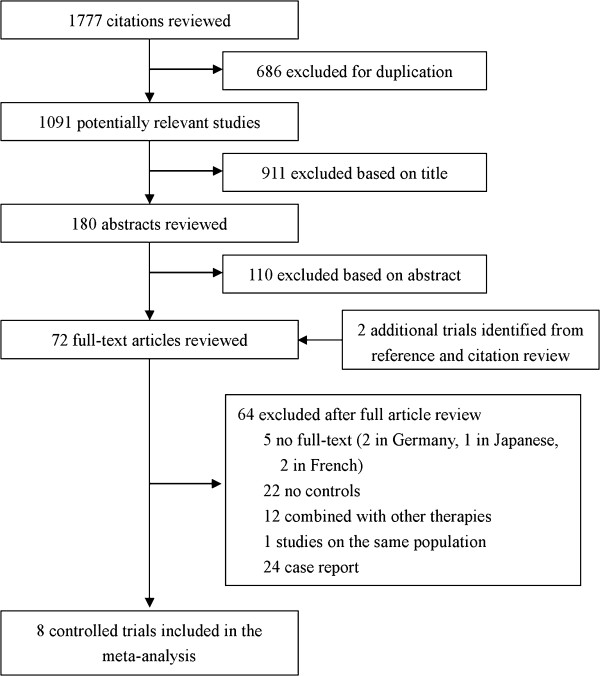
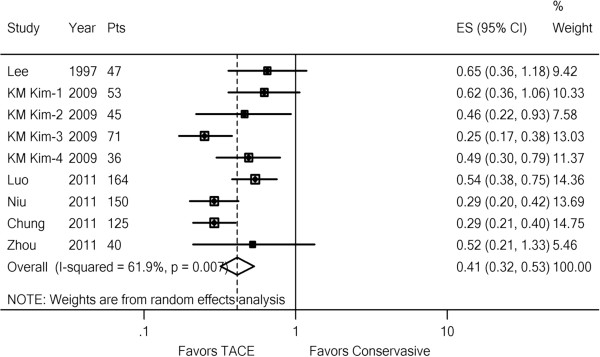
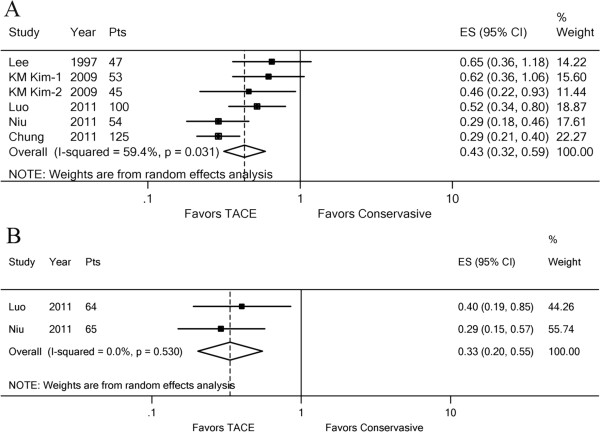
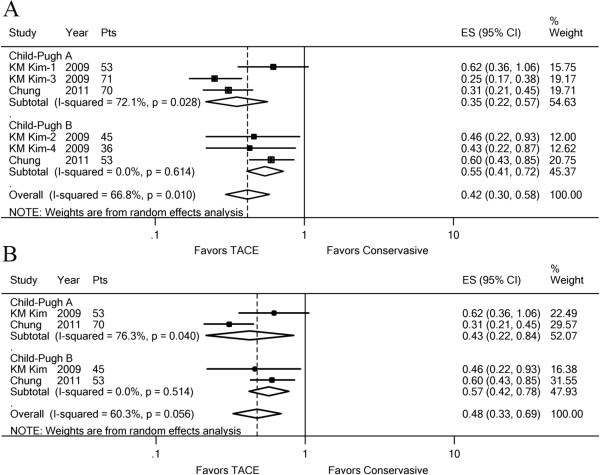
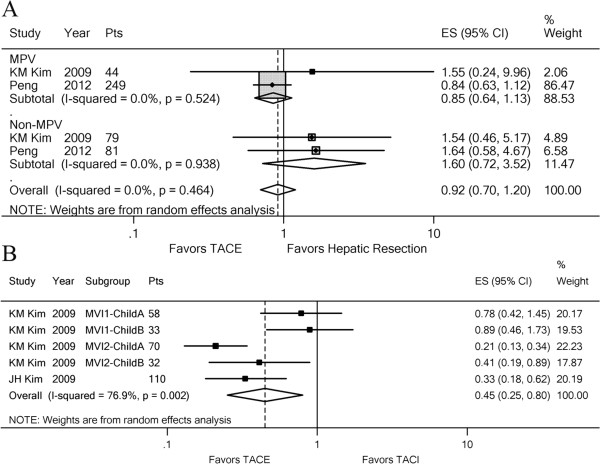
Results: Eight controlled trials involving 1601 HCC patients were included. TACE significantly improved the 6-month (HR, 0.41; 95% CI: 0.32-0.53; z, 6.28; p = 0.000) and 1-year (HR, 0.44; 95% CI: 0.34-0.57; z, 6.22; p = 0.000) overall survival of patients with PVTT compared with conservative treatment. Subgroup analyses showed that TACE was significantly effective in HCC patients whether with main portal vein (MPV) obstruction or with segmental PVTT. Fatal complications were rare, even in patients with MPV obstruction. Temporary liver decompensation and postembolization syndrome occurred frequently. However, they could be treated successfully with conservative treatment.
Conclusions: TACE, as a safe treatment, has potential for incurring a survival benefit for advanced HCC with PVTT, even with MPV obstruction. Further large randomized controlled trials may be needed to confirm this result.
Figures
References
-
- Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, Luo R, Feng J, Ye S, Yang TS. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10:25–34. doi: 10.1016/S1470-2045(08)70285-7. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
