

Calcitriol, calcidiol, parathyroid hormone, and fibroblast growth factor-23 interactions in chronic kidney disease
- PMID: 23566108
- PMCID: PMC3677418
- DOI: 10.1111/vec.12036
Calcitriol, calcidiol, parathyroid hormone, and fibroblast growth factor-23 interactions in chronic kidney disease
Abstract
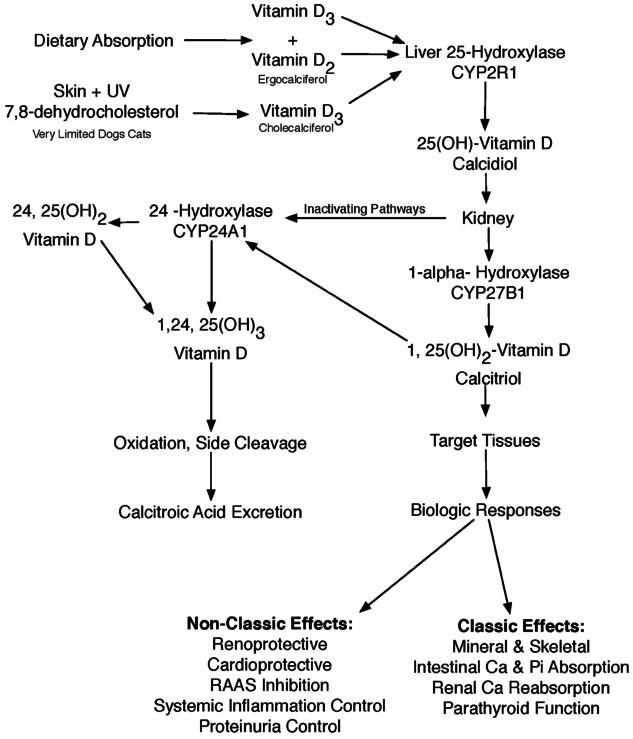
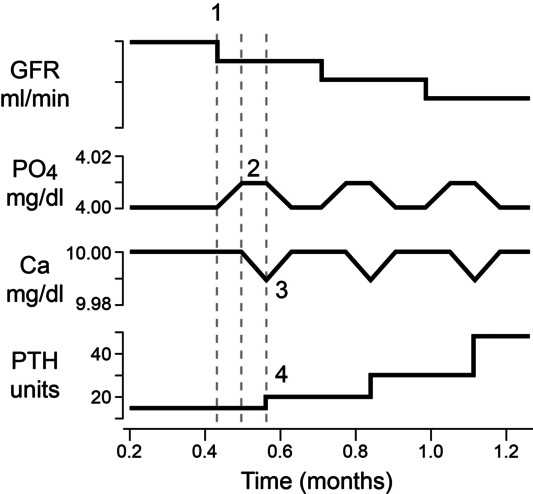
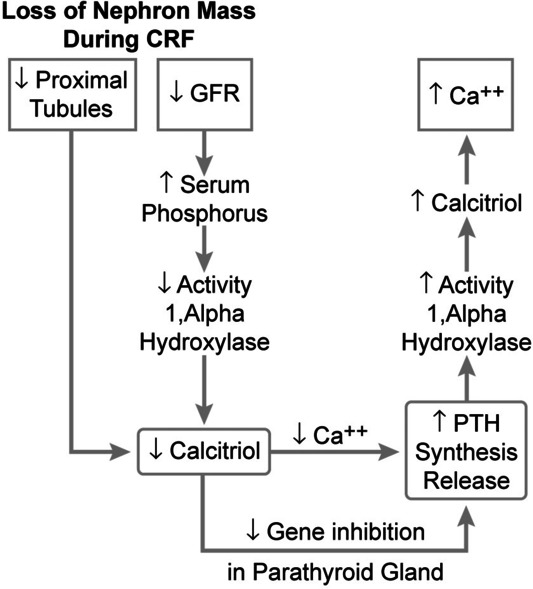
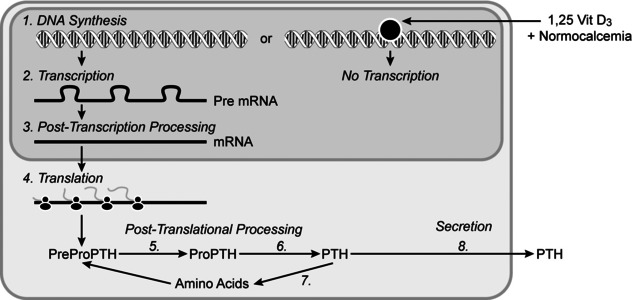
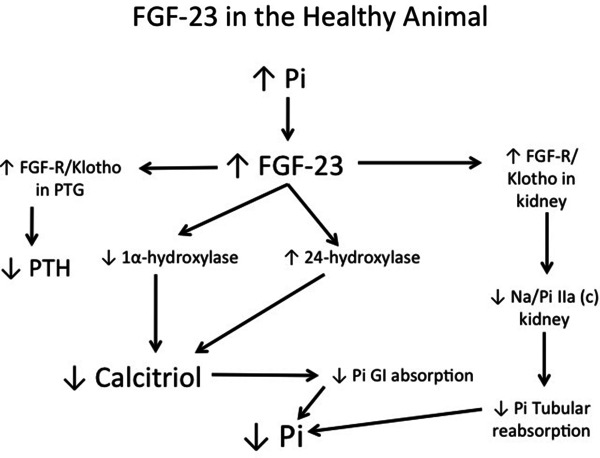
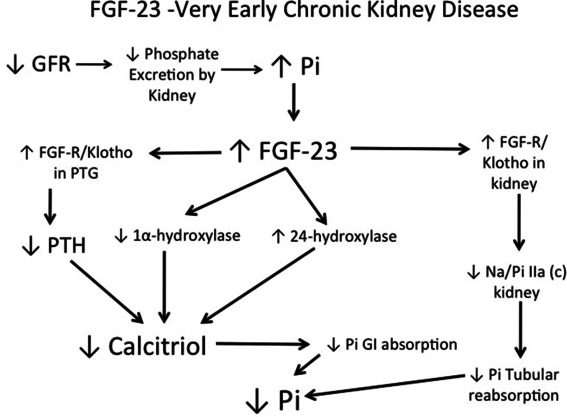
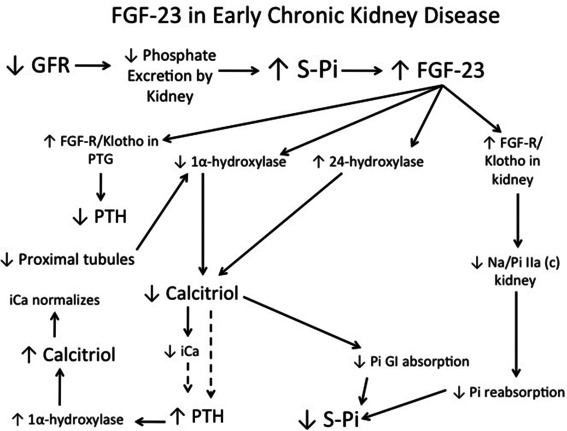
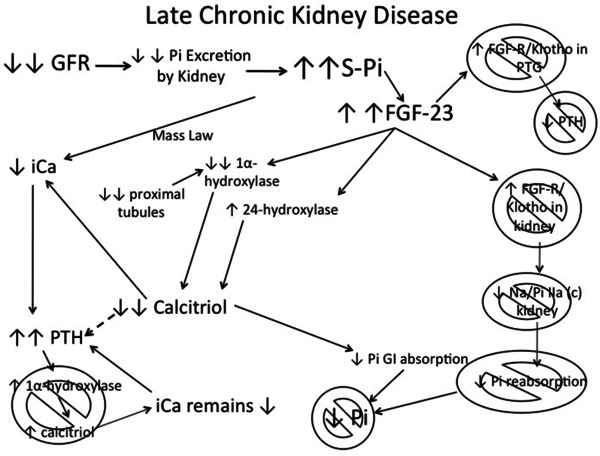
Objective: To review the inter-relationships between calcium, phosphorus, parathyroid hormone (PTH), parent and activated vitamin D metabolites (vitamin D, 25(OH)-vitamin D, 1,25(OH)2 -vitamin D, 24,25(OH)2 -vitamin D), and fibroblast growth factor-23 (FGF-23) during chronic kidney disease (CKD) in dogs and cats.
Data sources: Human and veterinary literature.
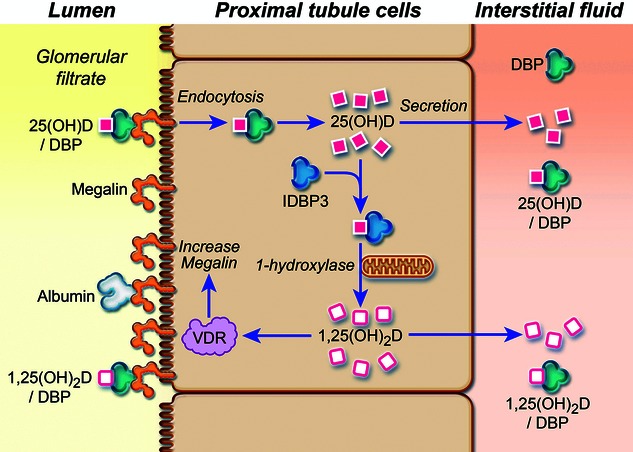
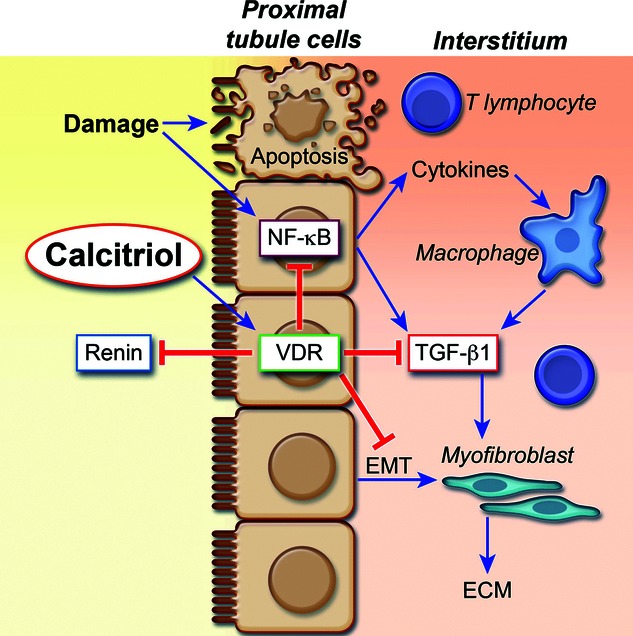
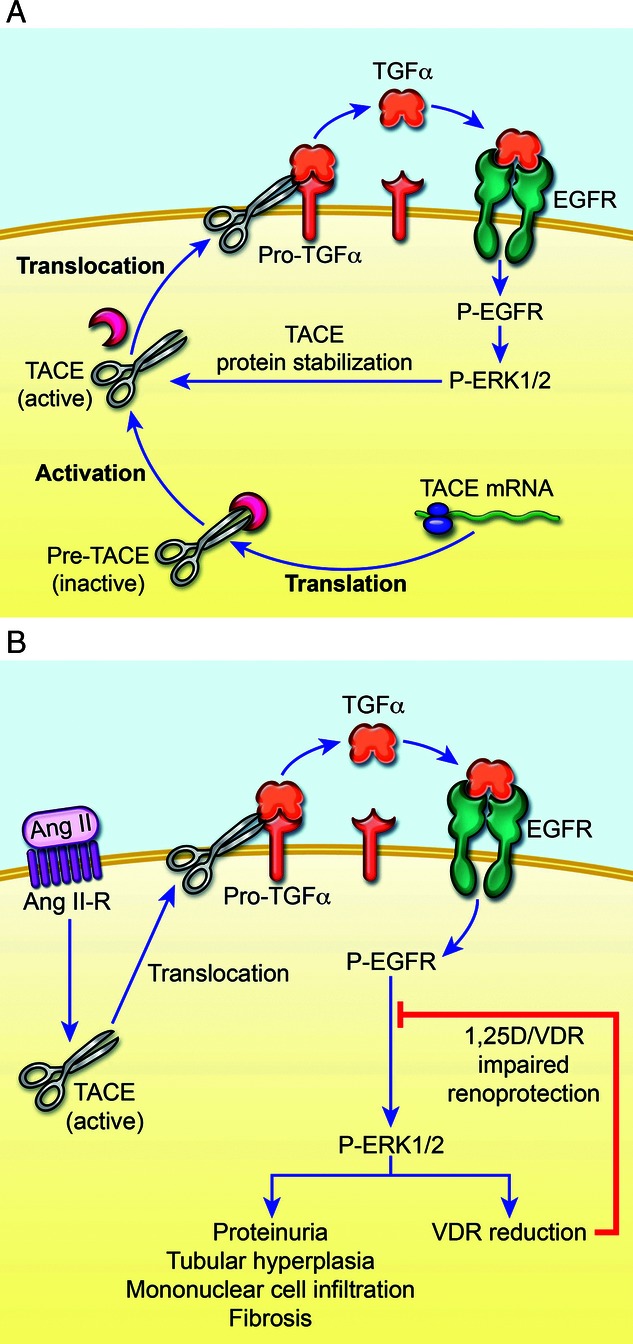
Human data synthesis: Beneficial effects of calcitriol treatment during CKD have traditionally been attributed to regulation of PTH but new perspectives emphasize direct renoprotective actions independent of PTH and calcium. It is now apparent that calcitriol exerts an important effect on renal tubular reclamation of filtered 25(OH)-vitamin D, which may be important in maintaining adequate circulating 25(OH)-vitamin D. This in turn may be vital for important pleiotropic actions in peripheral tissues through autocrine/paracrine mechanisms that impact the health of those local tissues.
Veterinary data synthesis: Limited information is available reporting the benefit of calcitriol treatment in dogs and cats with CKD.
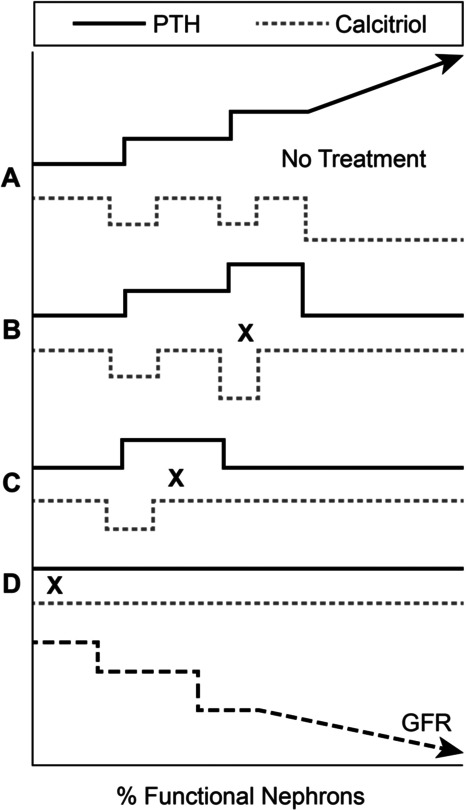
Conclusions: A survival benefit has been shown for dogs with CKD treated with calcitriol compared to placebo. The concentrations of circulating 25(OH)-vitamin D have recently been shown to be low in people and dogs with CKD and are related to survival in people with CKD. Combination therapy for people with CKD using both parental and activated vitamin D compounds is common in human nephrology and there is a developing emphasis using combination treatment with activated vitamin D and renin-angiotensin-aldosterone-system (RAAS) inhibitors.
© Veterinary Emergency and Critical Care Society 2013.
Figures
Similar articles
-
Association of Vitamin D Metabolites with Parathyroid Hormone, Fibroblast Growth Factor-23, Calcium, and Phosphorus in Dogs with Various Stages of Chronic Kidney Disease.J Vet Intern Med. 2017 May;31(3):791-798. doi: 10.1111/jvim.14653. Epub 2017 Feb 10. J Vet Intern Med. 2017. PMID: 28186657 Free PMC article.
-
Effects of calcifediol supplementation on markers of chronic kidney disease-mineral and bone disorder in dogs with chronic kidney disease.J Vet Intern Med. 2020 Nov;34(6):2497-2506. doi: 10.1111/jvim.15949. Epub 2020 Oct 31. J Vet Intern Med. 2020. PMID: 33128421 Free PMC article.
-
[Changes in mineral metabolism in stage 3, 4, and 5 chronic kidney disease (not on dialysis)].Nefrologia. 2008;28 Suppl 3:67-78. Nefrologia. 2008. PMID: 19018742 Spanish.
-
[Pathologies of calcium-phosphate homeostasis].Postepy Biochem. 2012;58(4):474-7. Postepy Biochem. 2012. PMID: 23662440 Review. Polish.
-
Regulatory mechanisms of circulating fibroblast growth factor 23 in parathyroid diseases.Ther Apher Dial. 2007 Oct;11 Suppl 1:S32-7. doi: 10.1111/j.1744-9987.2007.00519.x. Ther Apher Dial. 2007. PMID: 17976083 Review.
Cited by
-
The Role of Vitamin D in Small Animal Bone Metabolism.Metabolites. 2020 Dec 3;10(12):496. doi: 10.3390/metabo10120496. Metabolites. 2020. PMID: 33287408 Free PMC article. Review.
-
Urinary Tamm-Horsfall protein, albumin, vitamin D-binding protein, and retinol-binding protein as early biomarkers of chronic kidney disease in dogs.Physiol Rep. 2017 Jun;5(11):e13262. doi: 10.14814/phy2.13262. Physiol Rep. 2017. PMID: 28576851 Free PMC article.
-
Maternal nutritional risk factors for pre-eclampsia incidence: findings from a narrative scoping review.Reprod Health. 2022 Sep 5;19(1):188. doi: 10.1186/s12978-022-01485-9. Reprod Health. 2022. PMID: 36064716 Free PMC article.
-
Effects of isoflavone and probiotic intake on calcium transport and bone metabolism biomarkers in female rats.Food Sci Nutr. 2023 Jul 23;11(10):6324-6335. doi: 10.1002/fsn3.3571. eCollection 2023 Oct. Food Sci Nutr. 2023. PMID: 37823105 Free PMC article.
-
Investigating the Effects of Diet-Induced Pre-Diabetes on the Functioning of Calcium-Regulating Organs in Male Sprague Dawley Rats: Effects on Selected Markers.Front Endocrinol (Lausanne). 2022 Jul 11;13:914189. doi: 10.3389/fendo.2022.914189. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35898447 Free PMC article.
References
-
- Chew DJ, Nagode LA, Carothers MA. Disorders of calcium: hypercalcemia and hypocalcemia. In: DiBartola SP, editor. Fluid Therapy in Small Animal Practice. 1st edn. Philadelphia, PA: W.B. Saunders; 1992. pp. 1116–1176.
-
- Rosol TJ, Chew DJ, Nagode LA, Capen CC. Pathophysiology of calcium metabolism. Vet Clin Pathol. 1995;24(2):49–63. - PubMed
-
- Rosol TJ, Capen CC. Pathophysiology of calcium, phosphorus, and magnesium metabolism in animals. Vet Clin North Am Small Anim Pract. 1996;26:1155–1184. - PubMed
-
- Schenck PA, Chew DJ, Nagode LA. Disorders of calcium: hypercalcemia and hypocalcemia. In: DiBartola SP, et al., editors. Fluid, Electrolyte, and Acid-base Disorders in Small Animal Practice. 4th edn. St. Louis, MO: Elsevier; 2011. pp. 120–194.
-
- DeLuca HF. Evolution of our understanding of vitamin D. Nutrit Rev. 2008;66(10 Suppl 2):S73–S87. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
