

Using MRI for assessing velopharyngeal structures and function
- PMID: 23566261
- PMCID: PMC4496581
- DOI: 10.1597/12-083
Using MRI for assessing velopharyngeal structures and function
Erratum in
-
Erratum.Cleft Palate Craniofac J. 2015 May;52(3):382. doi: 10.1597/1545-1569-52.3.382. Cleft Palate Craniofac J. 2015. PMID: 25919361 No abstract available.
Abstract
Objective: Direct visualization of the velopharynx and, in particular, the levator muscle is particularly important in the assessment of velopharyngeal function and normal speech production. The purpose of this study is to demonstrate the development of a static and dynamic magnetic resonance imaging protocol for evaluation of velopharyngeal structures and function.
Methods: A high-resolution, T2-weighted turbo-spin-echo three-dimensional anatomical scan (sampling perfection with application optimized contrasts using different flip angle evolution) was used to acquire a large field of view covering the velopharyngeal anatomy. Dynamic speech assessment was obtained using a fast-gradient echo, fast low-angle shot, multi-shot spiral technique to acquire 15.8 frames per second (FPS) of the sagittal and oblique coronal image planes.
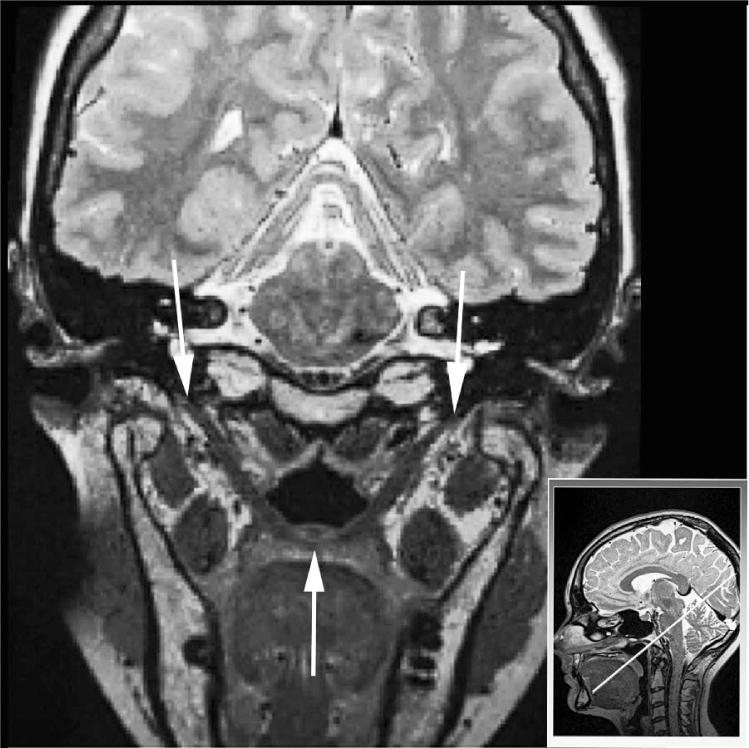
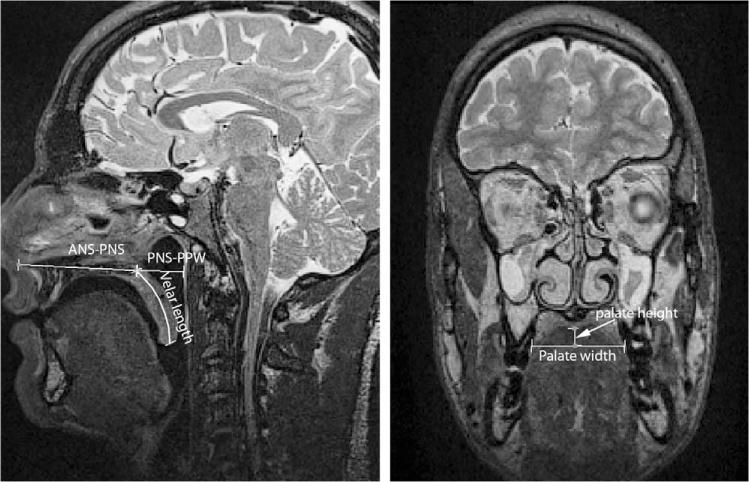
Results: Using a three-dimensional data set, as opposed to two-dimensional data, the full contour of the levator muscle can be appreciated. Dynamic images were obtained at 15.8 FPS in the sagittal and oblique coronal planes, enabling visualization of the movements of the velum, posterior pharyngeal wall, lateral pharyngeal walls, and levator muscle during speech.
Conclusions: A three-dimensional magnetic resonance imaging sequence, such as that used in the present study, may provide better analyses and more precise measurements. A dynamic fast low-angle shot sequence allows for visualization of the levator muscle and the velum during speech at a high image rate. This protocol could have a significant impact in improving the process of visualizing pathology and promoting clinical treatment plans for individuals born with cleft lip and palate.
Keywords: MRI; cleft palate; dynamic MRI during speech.
Figures


References
-
- Akgüner M. Velopharyngeal anthropometric analysis with MRI in normal subjects. Ann Plast Surg. 1999;43:142–147. - PubMed
-
- Akgüner M, Karaca C, Barutçu¸ A, Özaksoy D, Yurt A, Vayvada H. Evaluation of velopharyngeal pathophysiology and velopharyngeal insufficiency with magnetic resonance imaging. Eur J Plast Surg. 1998;21:118–128.
-
- Anagnostara A, Stoeckli S, Weber OM, Kollias MD. Evaluation of the anatomical and functional properties of deglutition with various kinetic high-speed MRI sequences. J Magn Reson Imaging. 2001;14:194–199. - PubMed
-
- Atik B, Bekerecioglu M, Tan O, Etik O, Davran R, Arslan H. Evaluation of dynamic magnetic resonance imaging in assessing velopharyngeal insufficiency during phonation. J Craniofac Surg. 2008;19:566–572. - PubMed
-
- Bae Y, Kuehn DK, Conway CA, Sutton BP. Real-time magnetic resonance imaging of velopharyngeal activity with simultaneous speech recordings. Cleft Palate Craniofac J. 2011a;48:695–707. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
