

Common syndromes of orthostatic intolerance
- PMID: 23569093
- PMCID: PMC3639459
- DOI: 10.1542/peds.2012-2610
Common syndromes of orthostatic intolerance
Abstract
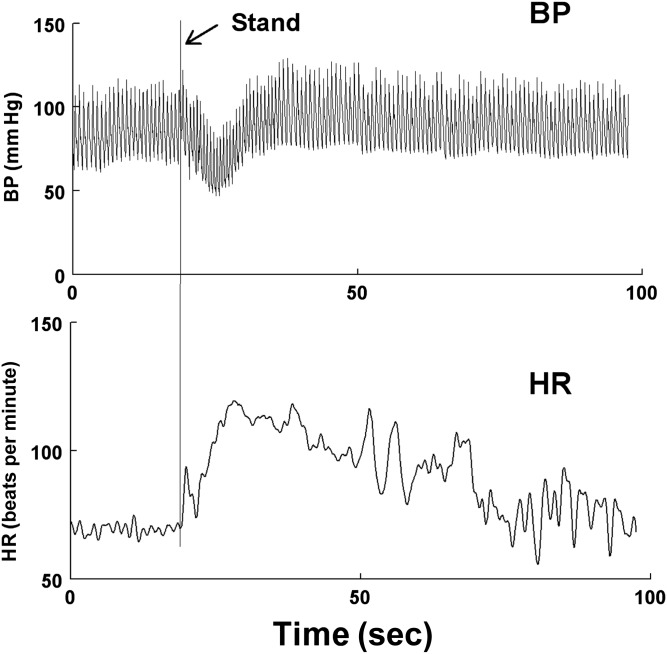
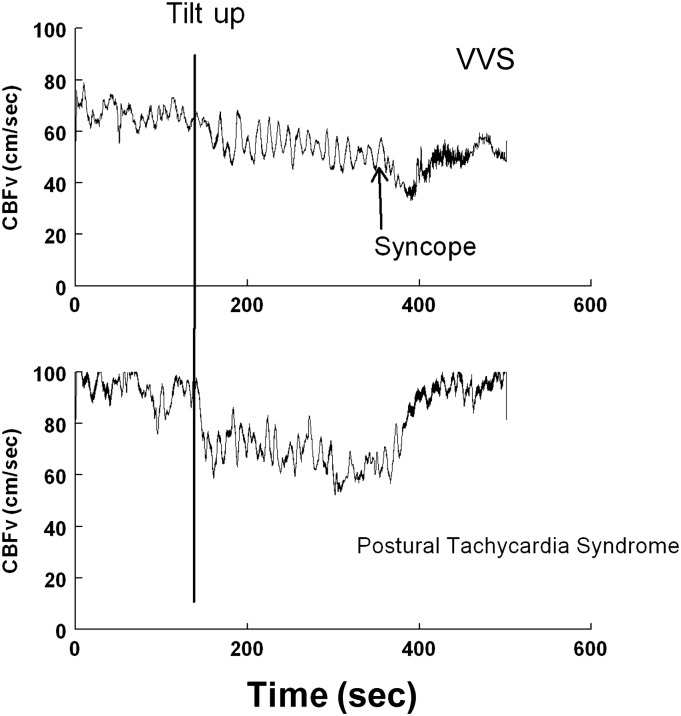
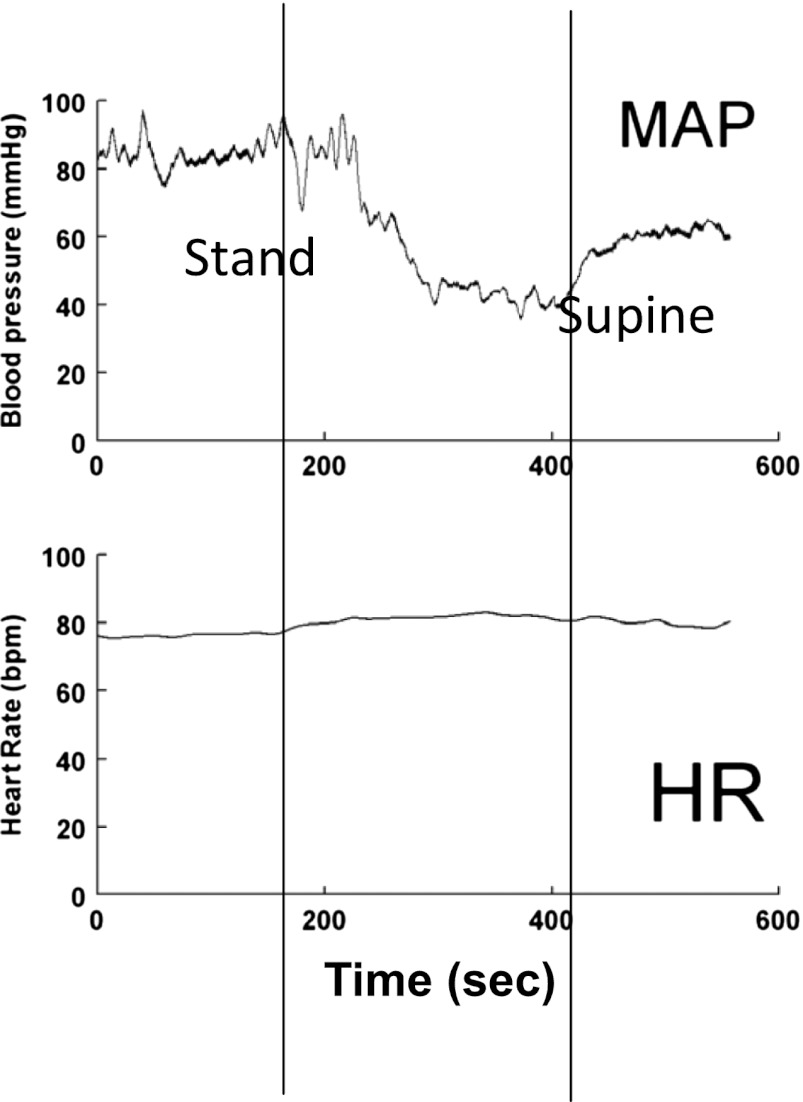
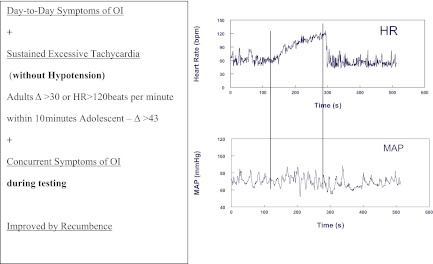
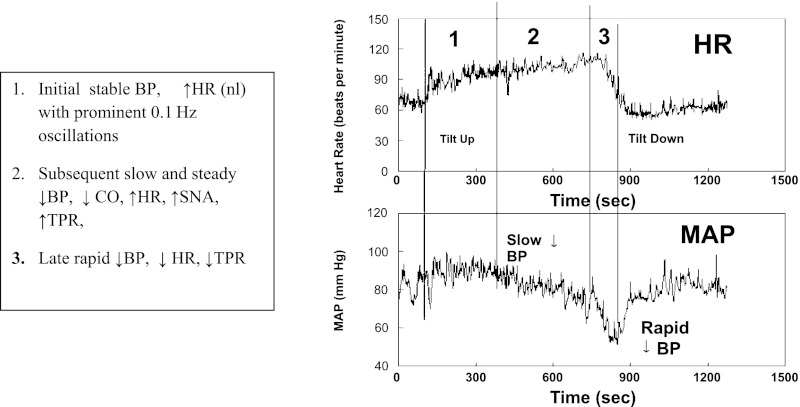
The autonomic nervous system, adequate blood volume, and intact skeletal and respiratory muscle pumps are essential components for rapid cardiovascular adjustments to upright posture (orthostasis). Patients lacking sufficient blood volume or having defective sympathetic adrenergic vasoconstriction develop orthostatic hypotension (OH), prohibiting effective upright activities. OH is one form of orthostatic intolerance (OI) defined by signs, such as hypotension, and symptoms, such as lightheadedness, that occur when upright and are relieved by recumbence. Mild OI is commonly experienced during intercurrent illnesses and when standing up rapidly. The latter is denoted "initial OH" and represents a normal cardiovascular adjustment to the blood volume shifts during standing. Some people experience episodic acute OI, such as postural vasovagal syncope (fainting), or chronic OI, such as postural tachycardia syndrome, which can significantly reduce quality of life. The lifetime incidence of ≥1 fainting episodes is ∼40%. For the most part, these episodes are benign and self-limited, although frequent syncope episodes can be debilitating, and injury may occur from sudden falls. In this article, mechanisms for OI having components of adrenergic hypofunction, adrenergic hyperfunction, hyperpnea, and regional blood volume redistribution are discussed. Therapeutic strategies to cope with OI are proposed.
Keywords: autonomic nervous system; hypocapnia; orthostatic hypotension; postural tachycardia syndrome; syncope.
Figures

References
-
- Rowell LB. Human Cardiovascular Control. New York, NY: Oxford University Press; 1993
-
- Thijs RD, Wieling W, van den Aardweg JG, van Dijk JG. Respiratory countermaneuvers in autonomic failure. Neurology. 2007;69(6):582–585 - PubMed
-
- van Dijk N, de Bruin IG, Gisolf J, et al. Hemodynamic effects of leg crossing and skeletal muscle tensing during free standing in patients with vasovagal syncope. J Appl Physiol. 2005;98(2):584–590 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
