

Load Balancing at Emergency Departments using 'Crowdinforming'
- PMID: 23569610
- PMCID: PMC3615787
- DOI: 10.5210/ojphi.v3i2.3520
Load Balancing at Emergency Departments using 'Crowdinforming'
Abstract
Background: Emergency Department (ED) overcrowding is an important healthcare issue facing increasing public and regulatory scrutiny in Canada and around the world. Many approaches to alleviate excessive waiting times and lengths of stay have been studied. In theory, optimal ED patient flow may be assisted via balancing patient loads between EDs (in essence spreading patients more evenly throughout this system). This investigation utilizes simulation to explore "Crowdinforming" as a basis for a process control strategy aimed to balance patient loads between six EDs within a mid-sized Canadian city.
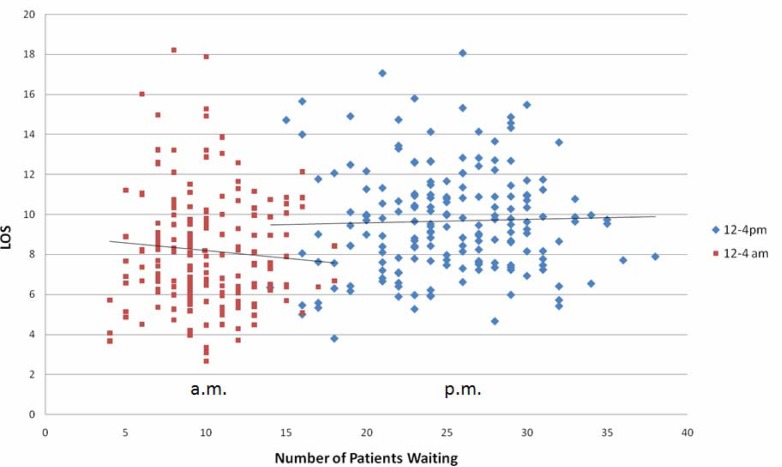
Methods: Anonymous patient visit data comprising 120,000 ED patient visits over six months to six ED facilities were obtained from the region's Emergency Department Information System (EDIS) to (1) determine trends in ED visits and interactions between parameters; (2) to develop a process control strategy integrating crowdinforming; and, (3) apply and evaluate the model in a simulated environment to explore the potential impact on patient self-redirection and load balancing between EDs.
Results: As in reality, the data available and subsequent model demonstrated that there are many factors that impact ED patient flow. Initial results suggest that for this particular data set used, ED arrival rates were the most useful metric for ED 'busyness' in a process control strategy, and that Emergency Department performance may benefit from load balancing efforts.
Conclusions: The simulation supports the use of crowdinforming as a potential tool when used in a process control strategy to balance the patient loads between EDs. The work also revealed that the value of several parameters intuitively expected to be meaningful metrics of ED 'busyness' was not evident, highlighting the importance of finding parameters meaningful within one's particular data set. The information provided in the crowdinforming model is already available in a local context at some ED sites. The extension to a wider dissemination of information via an Internet web service accessible by smart phones is readily achievable and not a technological obstacle. Similarly, the system could be extended to help direct patients by including future estimates or predictions in the crowdinformed data. The contribution of the simulation is to allow for effective policy evaluation to better inform the public of ED 'busyness' as part of their decision making process in attending an emergency department. In effect, this is a means of providing additional decision support insights garnered from a simulation, prior to a real world implementation.
Figures






Similar articles
-
Agent based modeling of "crowdinforming" as a means of load balancing at emergency departments.Online J Public Health Inform. 2010;2(3):ojphi.v2i3.3225. doi: 10.5210/ojphi.v2i3.3225. Epub 2010 Dec 23. Online J Public Health Inform. 2010. PMID: 23569589 Free PMC article.
-
The Impact of Ambulance and Patient Diversion on Crowdedness of Multiple Emergency Departments in a Region.PLoS One. 2015 Dec 11;10(12):e0144227. doi: 10.1371/journal.pone.0144227. eCollection 2015. PLoS One. 2015. PMID: 26659589 Free PMC article.
-
Development and Evaluation of a Virtual Research Environment to Improve Quality of Care in Overcrowded Emergency Departments: Observational Study.JMIR Serious Games. 2019 Aug 8;7(3):e13993. doi: 10.2196/13993. JMIR Serious Games. 2019. PMID: 31397292 Free PMC article.
-
Exploring parents' reasons for attending the emergency department for children with minor illnesses: a mixed methods systematic review.Emerg Med J. 2019 Jan;36(1):39-46. doi: 10.1136/emermed-2017-207118. Epub 2018 Nov 2. Emerg Med J. 2019. PMID: 30389792
-
Emergency Department Overcrowding in Canada: CADTH Health Technology Review Recommendation [Internet].Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2023 Nov. Report No.: OP0553GUI. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2023 Nov. Report No.: OP0553GUI. PMID: 38320069 Free Books & Documents. Review.
Cited by
-
Breaking the Emergency Room Cycle: The Impact of Telemedicine on Emergency Department Utilization.Cureus. 2024 Mar 3;16(3):e55457. doi: 10.7759/cureus.55457. eCollection 2024 Mar. Cureus. 2024. PMID: 38571862 Free PMC article.
-
Equity distribution of quality evaluation reports to doctors in health care organizations.PeerJ Comput Sci. 2022 Jan 21;8:e819. doi: 10.7717/peerj-cs.819. eCollection 2022. PeerJ Comput Sci. 2022. PMID: 35174262 Free PMC article.
-
Assessing time to treatment and patient inflow in a Danish emergency department: a cohort study using data from electronic emergency screen boards.BMC Res Notes. 2014 Oct 6;7:690. doi: 10.1186/1756-0500-7-690. BMC Res Notes. 2014. PMID: 25288356 Free PMC article.
-
Studying the Variability in Patient Inflow and Staffing Trends on Sundays versus Other Days in the Academic Emergency Department.J Emerg Trauma Shock. 2017 Jul-Sep;10(3):121-127. doi: 10.4103/JETS.JETS_139_16. J Emerg Trauma Shock. 2017. PMID: 28855774 Free PMC article.
References
-
- Thompson DA, Yarnold PR, Williams DR, Adams SL. Effects of actual waiting time, perceived waiting time, information delivery, and expressive quality on patient satisfaction in the emergency department. Ann Emerg Med. 1996;28:657–665. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
