

CXCL13 plus interleukin 10 is highly specific for the diagnosis of CNS lymphoma
- PMID: 23570798
- PMCID: PMC3674672
- DOI: 10.1182/blood-2013-01-476333
CXCL13 plus interleukin 10 is highly specific for the diagnosis of CNS lymphoma
Abstract
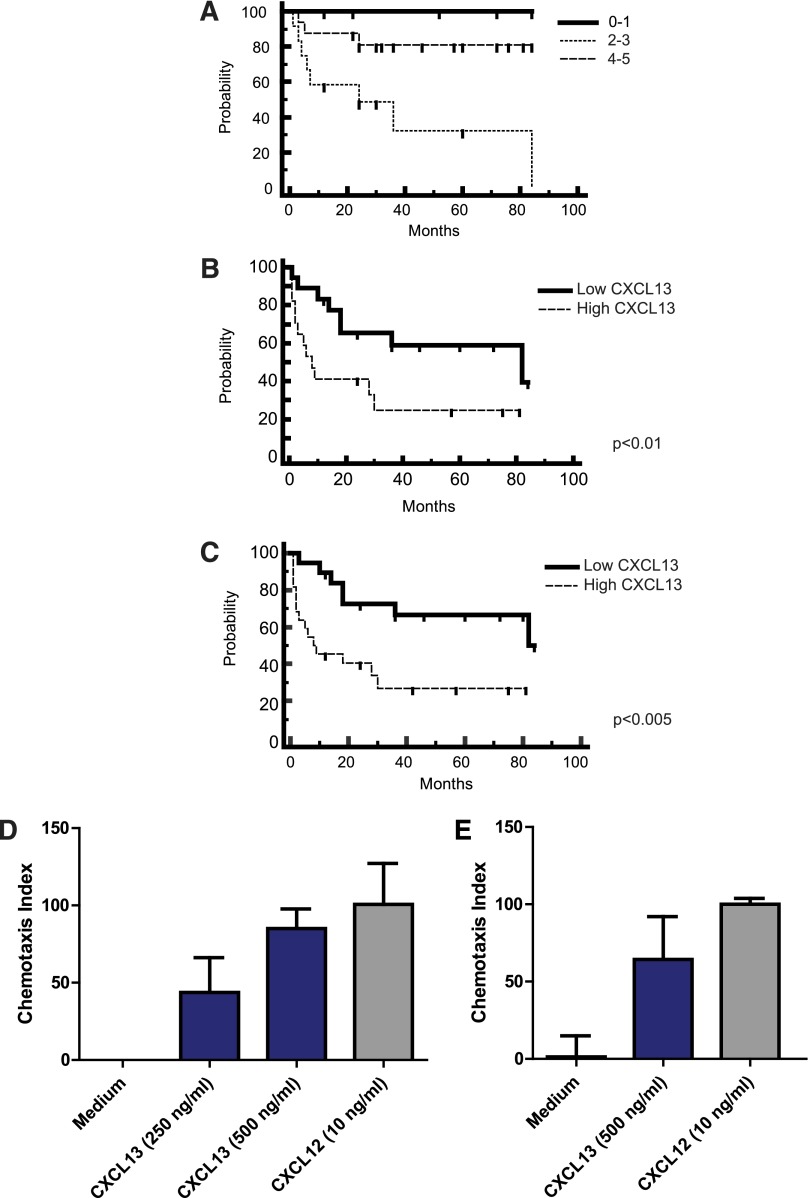
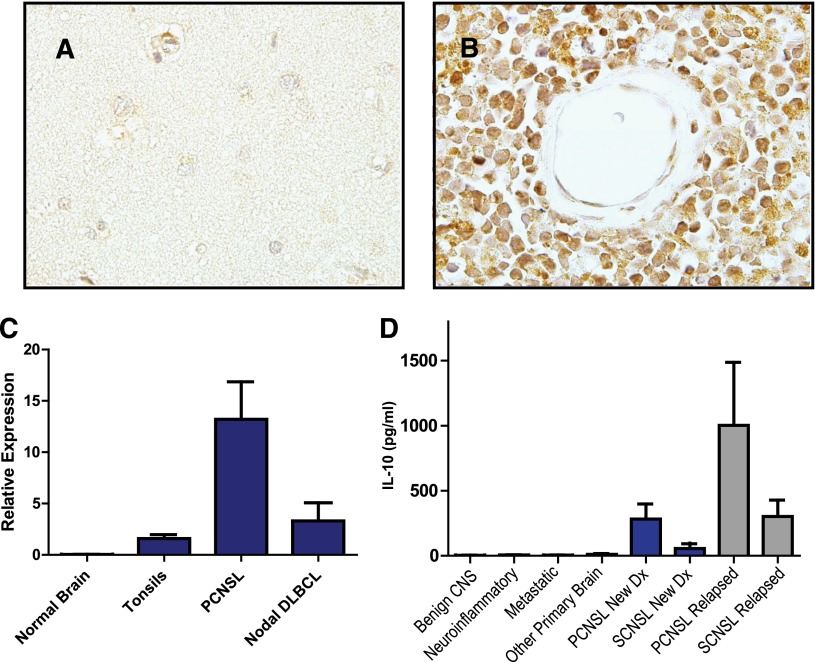
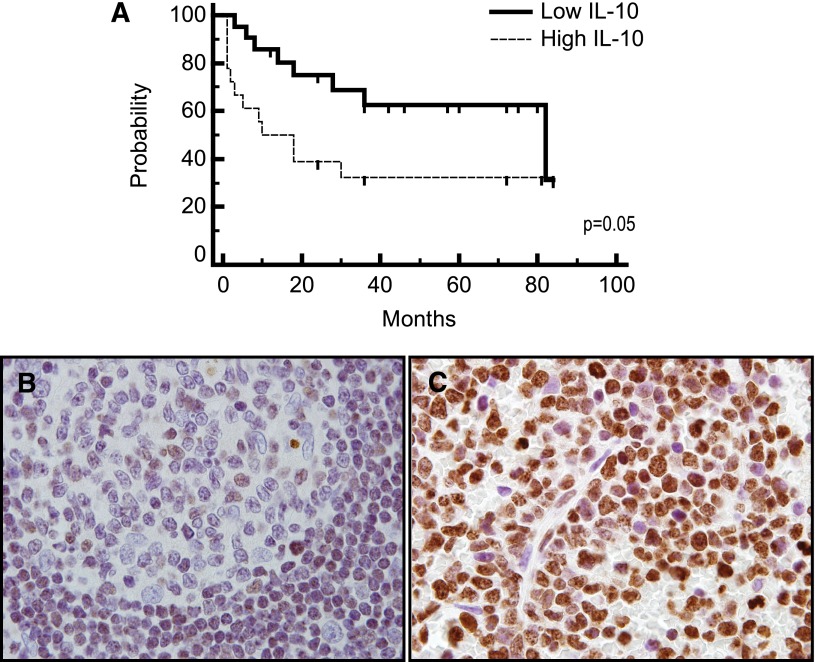
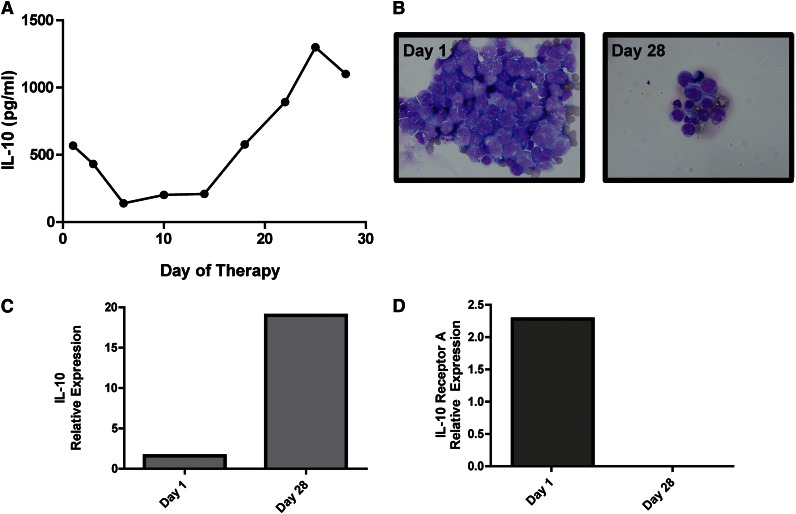
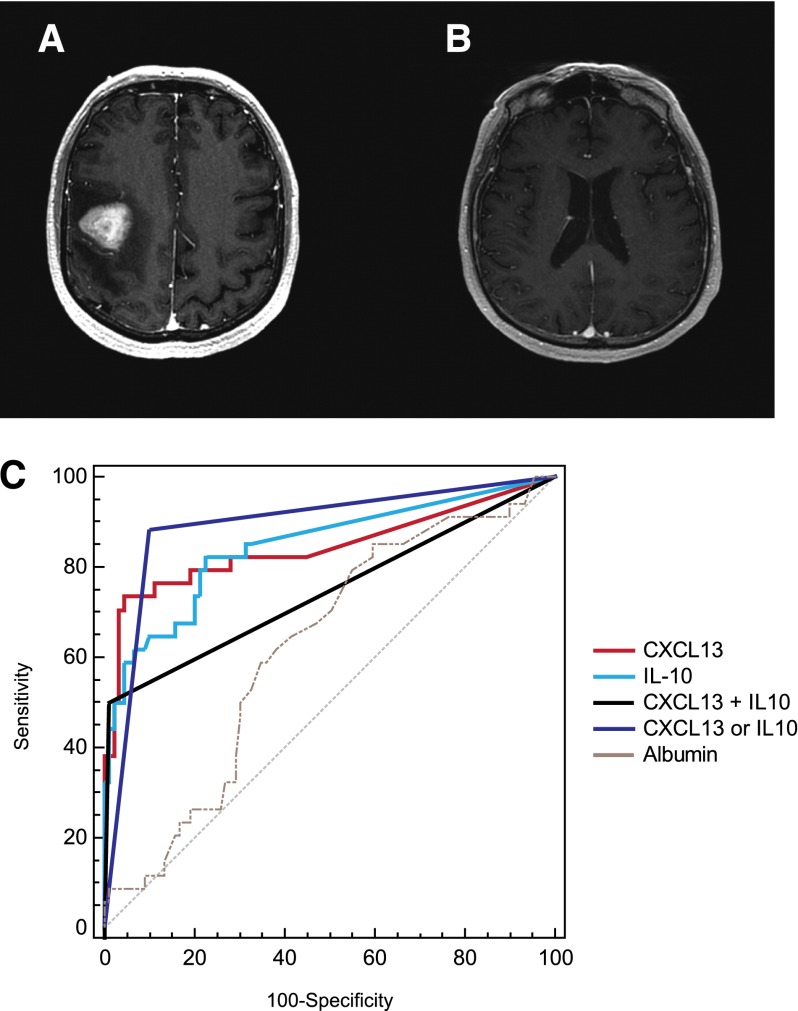
Establishing the diagnosis of focal brain lesions in patients with unexplained neurologic symptoms represents a challenge. The goal of this study is to provide evidence supporting functional roles for CXC chemokine ligand (CXCL)13 and interleukin (IL)-10 in central nervous system (CNS) lymphomas and to evaluate the utility of each as prognostic and diagnostic biomarkers. We demonstrate for the first time that elevated CXCL13 concentration in cerebrospinal fluid (CSF) is prognostic and that CXCL13 and CXCL12 mediate chemotaxis of lymphoma cells isolated from CNS lymphoma lesions. Expression of the activated form of Janus kinase 1 supported a role for IL-10 in prosurvival signaling. We determined the concentration of CXCL13 and IL-10 in CSF of CNS lymphoma patients and control cohorts including inflammatory and degenerative neurologic disease in a multicenter study involving 220 patients. Bivariate elevated CXCL13 plus IL-10 was 99.3% specific for primary and secondary CNS lymphoma, with sensitivity significantly greater than reference standard CSF tests. These results identify CXCL13 and IL-10 as potentially important biomarkers of CNS lymphoma that merit further evaluation and support incorporation of CXCL13 and IL-10 into diagnostic algorithms for the workup of focal brain lesions in which lymphoma is a consideration.
Figures

References
-
- Josephson SA, Papanastassiou AM, Berger MS, et al. The diagnostic utility of brain biopsy procedures in patients with rapidly deteriorating neurological conditions or dementia. J Neurosurg. 2007;106(1):72–75. - PubMed
-
- Hall WA. The safety and efficacy of stereotactic biopsy for intracranial lesions. Cancer. 1998;82(9):1749–1755. - PubMed
-
- Javedan SP, Tamargo RJ. Diagnostic yield of brain biopsy in neurodegenerative disorders. Neurosurgery. 1997;41(4):823–828, discussion 828-830. - PubMed
-
- Ferreri AJ. How I treat primary CNS lymphoma. Blood. 2011;118(3):510–522. - PubMed
-
- Hormigo A, Abrey L, Heinemann MH, DeAngelis LM. Ocular presentation of primary central nervous system lymphoma: diagnosis and treatment. Br J Haematol. 2004;126(2):202–208. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
