

Role of late sodium current as a potential arrhythmogenic mechanism in the progression of pressure-induced heart disease
- PMID: 23570977
- PMCID: PMC3720777
- DOI: 10.1016/j.yjmcc.2013.03.021
Role of late sodium current as a potential arrhythmogenic mechanism in the progression of pressure-induced heart disease
Abstract
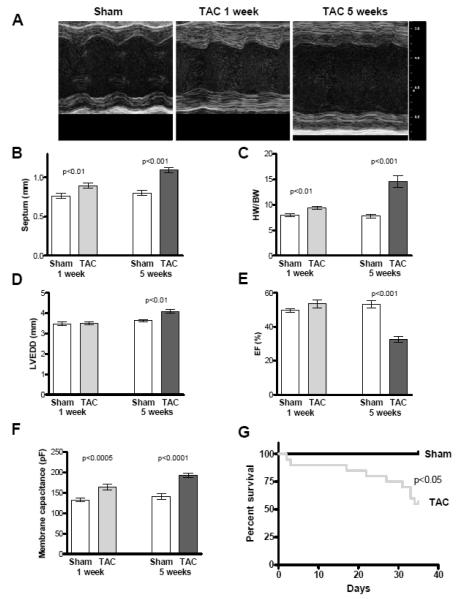
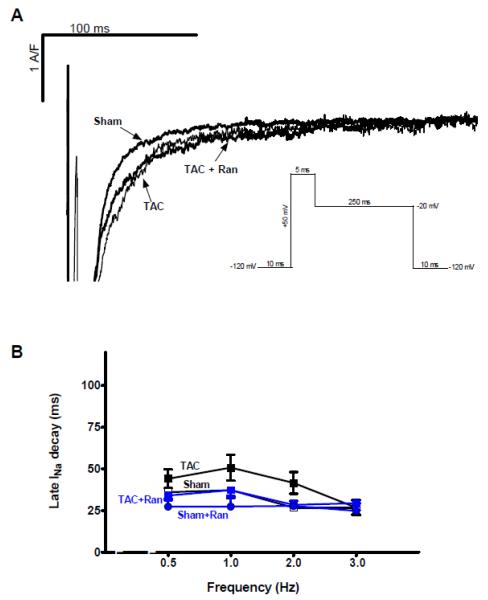
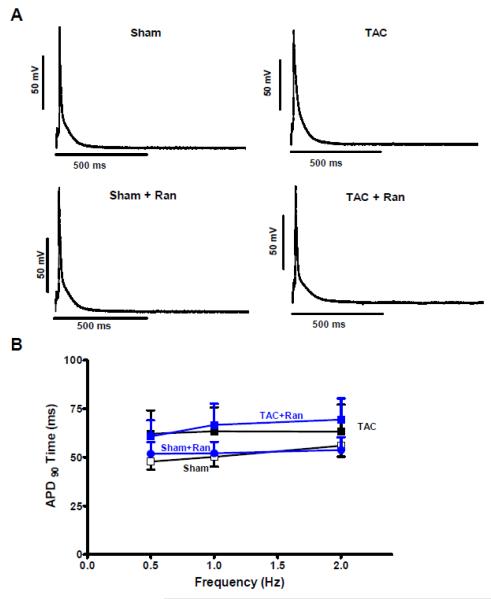
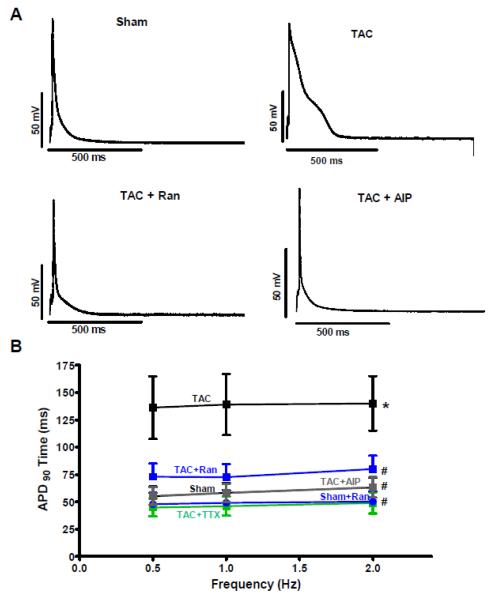
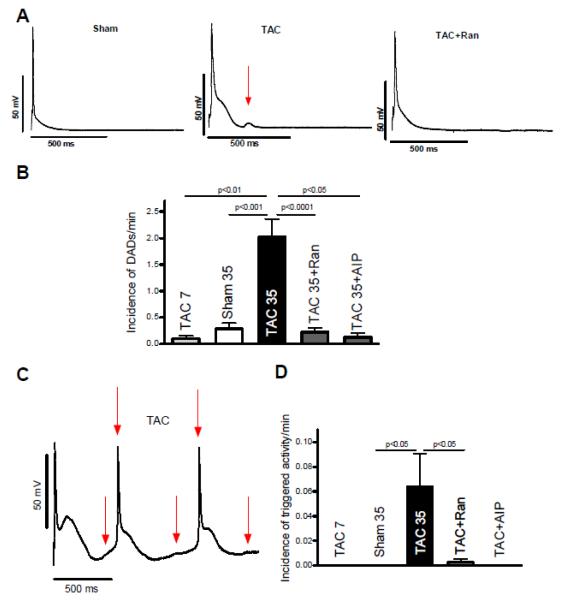
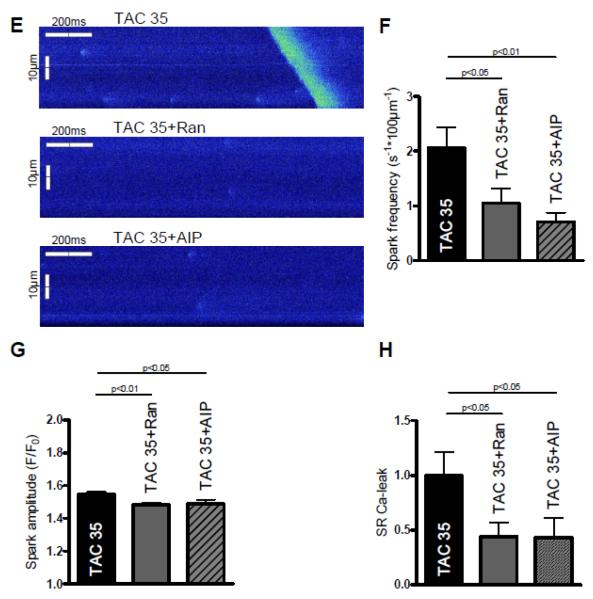
The aim of the study was to determine the characteristics of the late Na current (INaL) and its arrhythmogenic potential in the progression of pressure-induced heart disease. Transverse aortic constriction (TAC) was used to induce pressure overload in mice. After one week the hearts developed isolated hypertrophy with preserved systolic contractility. In patch-clamp experiments both, INaL and the action potential duration (APD90) were unchanged. In contrast, after five weeks animals developed heart failure with prolonged APDs and slowed INaL decay time which could be normalized by addition of the INaL inhibitor ranolazine (Ran) or by the Ca/calmodulin-dependent protein kinase II (CaMKII) inhibitor AIP. Accordingly the APD90 could be significantly abbreviated by Ran, tetrodotoxin and the CaMKII inhibitor AIP. Isoproterenol increased the number of delayed afterdepolarizations (DAD) in myocytes from failing but not sham hearts. Application of either Ran or AIP prevented the occurrence of DADs. Moreover, the incidence of triggered activity was significantly increased in TAC myocytes and was largely prevented by Ran and AIP. Western blot analyses indicate that increased CaMKII activity and a hyperphosphorylation of the Nav1.5 at the CaMKII phosphorylation site (Ser571) paralleled our functional observations five weeks after TAC surgery. In pressure overload-induced heart failure a CaMKII-dependent augmentation of INaL plays a crucial role in the AP prolongation and generation of cellular arrhythmogenic triggers, which cannot be found in early and still compensated hypertrophy. Inhibition of INaL and CaMKII exerts potent antiarrhythmic effects and might therefore be of potential therapeutic interest. This article is part of a Special Issue entitled "Na(+) Regulation in Cardiac Myocytes".
Keywords: Arrhythmias; CaMKII; Heart failure; Hypertrophy; I(NaL); Ranolazine.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures


References
-
- Bers DM. Excitation-Contraction Coupling and Cardiac Contractile Force. 2nd ed Kluwer Academic Publishers; Dordrecht, Netherlands: 2001.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
