

Screening for precancerous lesions of upper gastrointestinal tract: from the endoscopists' viewpoint
- PMID: 23573079
- PMCID: PMC3615623
- DOI: 10.1155/2013/681439
Screening for precancerous lesions of upper gastrointestinal tract: from the endoscopists' viewpoint
Abstract
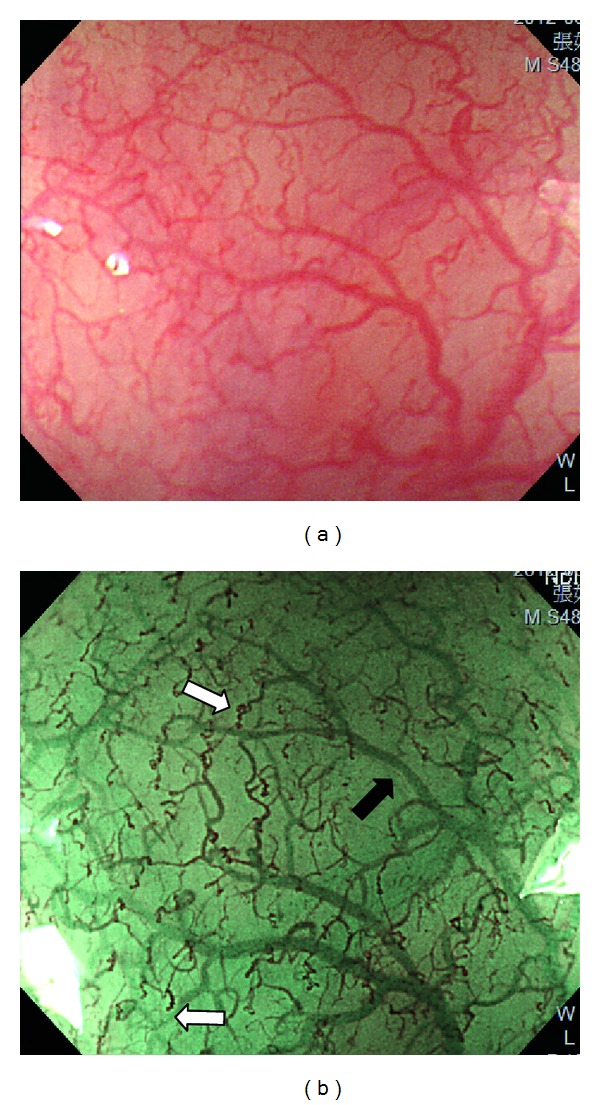
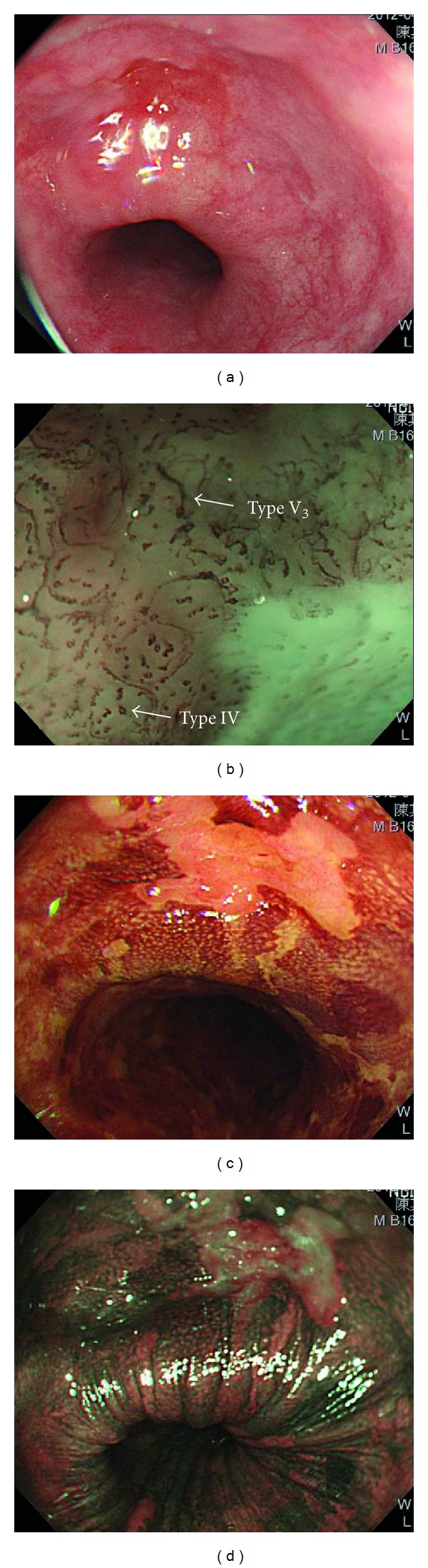
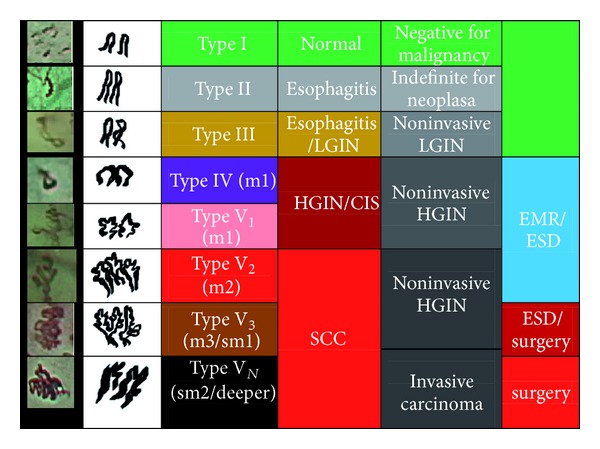
Upper gastrointestinal tract cancers are one of the most important leading causes of cancer death worldwide. Diagnosis at late stages always brings about poor outcome of these malignancies. The early detection of precancerous or early cancerous lesions of gastrointestinal tract is therefore of utmost importance to improve the overall outcome and maintain a good quality of life of patients. The desire of endoscopists to visualize the invisibles under conventional white-light endoscopy has accelerated the advancements in endoscopy technologies. Nowadays, image-enhanced endoscopy which utilizes optical- or dye-based contrasting techniques has been widely applied in endoscopic screening program of gastrointestinal tract malignancies. These contrasting endoscopic technologies not only improve the visualization of early foci missed by conventional endoscopy, but also gain the insight of histopathology and tumor invasiveness, that is so-called optical biopsy. Here, we will review the application of advanced endoscopy technique in screening program of upper gastrointestinal tract cancers.
Figures

Similar articles
-
Deep learning for diagnosis of precancerous lesions in upper gastrointestinal endoscopy: A review.World J Gastroenterol. 2021 May 28;27(20):2531-2544. doi: 10.3748/wjg.v27.i20.2531. World J Gastroenterol. 2021. PMID: 34092974 Free PMC article. Review.
-
Advances in optical gastrointestinal endoscopy: a technical review.Mol Oncol. 2021 Oct;15(10):2580-2599. doi: 10.1002/1878-0261.12792. Epub 2020 Sep 19. Mol Oncol. 2021. PMID: 32915503 Free PMC article. Review.
-
Is image-enhanced endoscopy useful for the diagnosis and treatment of gastrointestinal tumor?Clin Endosc. 2013 May;46(3):248-50. doi: 10.5946/ce.2013.46.3.248. Epub 2013 May 31. Clin Endosc. 2013. PMID: 23767035 Free PMC article.
-
Real-time artificial intelligence for detection of upper gastrointestinal cancer by endoscopy: a multicentre, case-control, diagnostic study.Lancet Oncol. 2019 Dec;20(12):1645-1654. doi: 10.1016/S1470-2045(19)30637-0. Epub 2019 Oct 4. Lancet Oncol. 2019. PMID: 31591062 Clinical Trial.
-
State of the art in advanced endoscopic imaging for the detection and evaluation of dysplasia and early cancer of the gastrointestinal tract.Clin Exp Gastroenterol. 2014 May 13;7:133-50. doi: 10.2147/CEG.S58157. eCollection 2014. Clin Exp Gastroenterol. 2014. PMID: 24868168 Free PMC article. Review.
Cited by
-
Screening and surveillance of esophageal cancer by magnifying endoscopy with narrow band imaging improves the survival of hypopharyngeal cancer patients.Front Oncol. 2024 Jan 23;13:1221616. doi: 10.3389/fonc.2023.1221616. eCollection 2023. Front Oncol. 2024. PMID: 38322289 Free PMC article.
-
Artificial Intelligence for Upper Gastrointestinal Endoscopy: A Roadmap from Technology Development to Clinical Practice.Diagnostics (Basel). 2022 May 21;12(5):1278. doi: 10.3390/diagnostics12051278. Diagnostics (Basel). 2022. PMID: 35626433 Free PMC article. Review.
-
Deep learning for diagnosis of precancerous lesions in upper gastrointestinal endoscopy: A review.World J Gastroenterol. 2021 May 28;27(20):2531-2544. doi: 10.3748/wjg.v27.i20.2531. World J Gastroenterol. 2021. PMID: 34092974 Free PMC article. Review.
-
hERG1 Potassium Channel Expression in Colorectal Adenomas: Comparison with Other Preneoplastic Lesions of the Gastrointestinal Tract.Curr Issues Mol Biol. 2022 Mar 17;44(3):1326-1331. doi: 10.3390/cimb44030089. Curr Issues Mol Biol. 2022. PMID: 35723312 Free PMC article.
-
Endoscopic Screening for Second Primary Tumors of the Esophagus Among Head and Neck Cancer Patients.Front Oncol. 2022 Jun 7;12:906125. doi: 10.3389/fonc.2022.906125. eCollection 2022. Front Oncol. 2022. PMID: 35747824 Free PMC article. Review.
References
-
- Bolye PLB. World Cancer Report. Lyon, France: IARC Press; 2008.
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA: Cancer Journal for Clinicians. 2011;61(2):69–90. - PubMed
-
- Wang KK, Sampliner RE. Updated guidelines 2008 for the diagnosis, surveillance and therapy of Barrett’s esophagus. American Journal of Gastroenterology. 2008;103(3):788–797. - PubMed
-
- Theisen J, Stein HJ, Dittler HJ, et al. Preoperative chemotherapy unmasks underlying Barrett’s mucosa in patients with adenocarcinoma of the distal esophagus. Surgical Endoscopy and Other Interventional Techniques. 2002;16(4):671–673. - PubMed
-
- Hvid-Jensen F, Pedersen L, Drewes AM, Sørensen HT, Funch-Jensen P. Incidence of adenocarcinoma among patients with Barrett’s esophagus. The New England Journal of Medicine. 2011;365(15):1375–1383. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
