

Outcomes of endoscopic-ultrasound-guided cholangiopancreatography: a literature review
- PMID: 23573080
- PMCID: PMC3614028
- DOI: 10.1155/2013/869214
Outcomes of endoscopic-ultrasound-guided cholangiopancreatography: a literature review
Abstract
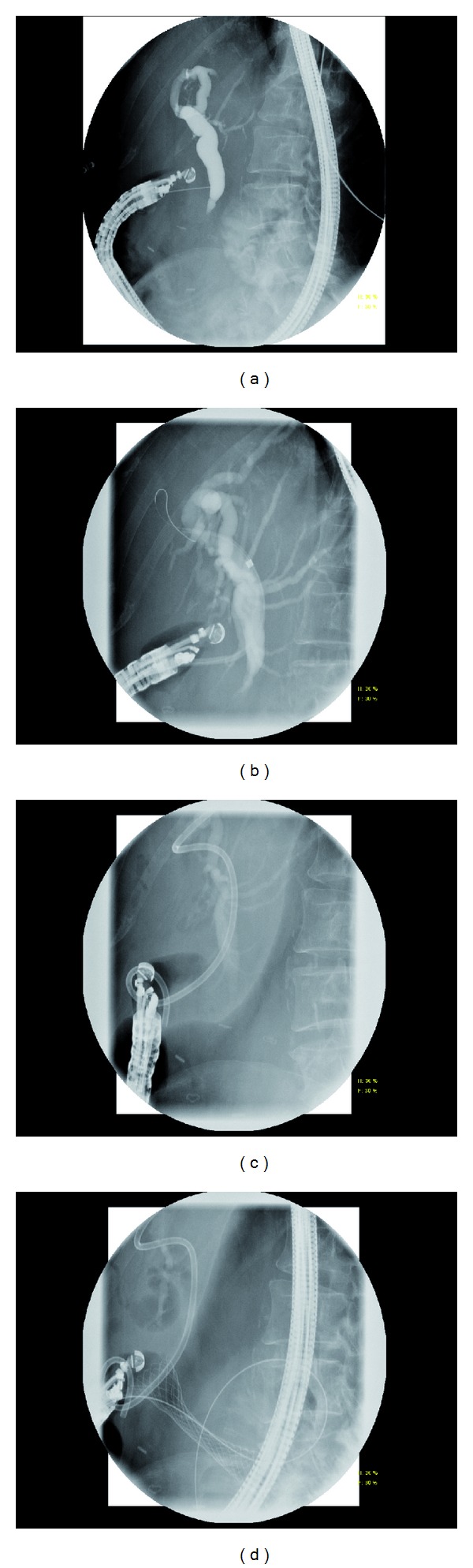
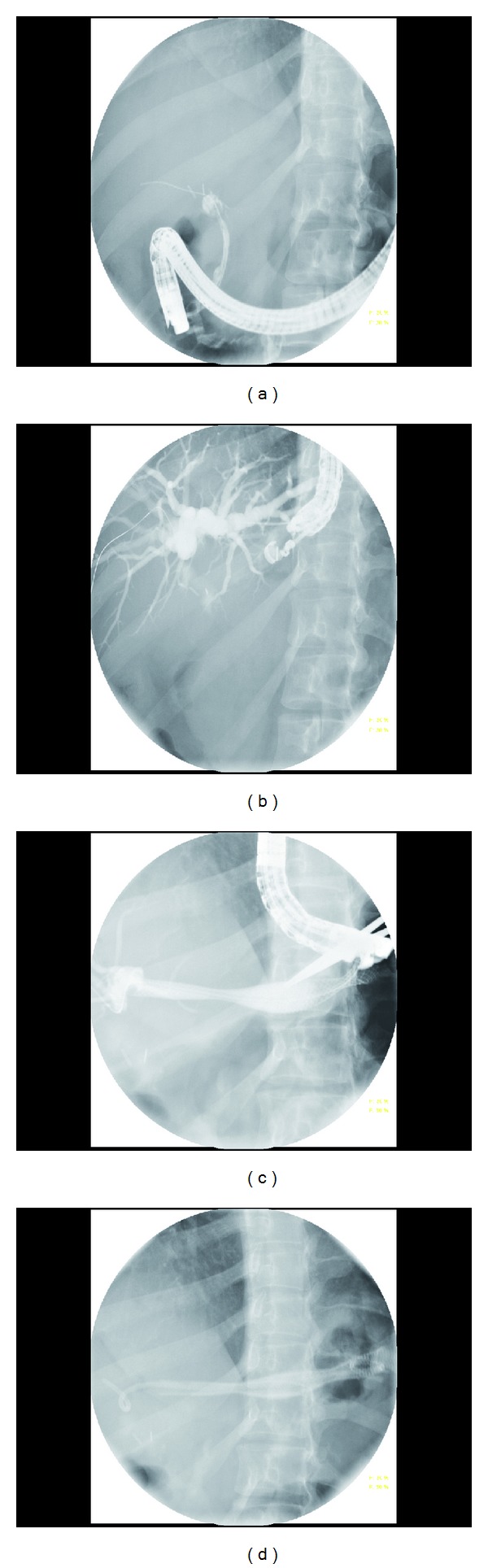
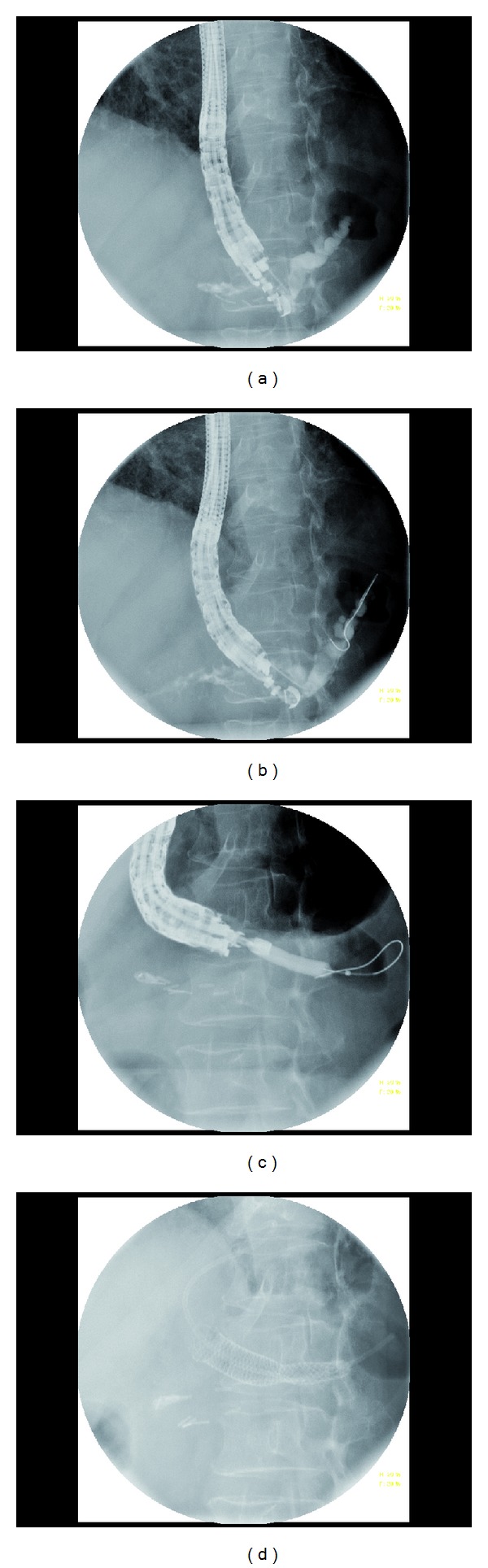
Endoscopic retrograde cholangiopancreatography (ERCP) can fail in 3-10% of the cases even in experienced hands. Although percutaneous transhepatic cholangiography (PTC) and surgery are the traditional alternatives, there are morbidity and mortality associated with both. In this paper, we have discussed the efficacy and safety of endoscopic-ultrasound-guided cholangiopancreatography (EUS-CP) in decompression of biliary and pancreatic ducts. The overall technical and clinical success rates are around 90% for biliary and 70% for pancreatic duct drainage. The overall EUS-CP complication rate is around 15%. EUS-CP is, however, a technically challenging procedure and should be performed by an experienced endoscopist skilled in both EUS and ERCP. Same session EUS-CP as failed initial ERCP is practical and may result in avoidance of additional procedures. With increasing availability of endoscopists trained in both ERCP and EUS, the role of EUS-CP is likely to grow in clinical practice.
Figures
References
-
- Huibregtse K, Kimmey MB. Endoscopic retrograde cholangiopancreatography, endoscopic sphincterotomy and endoscopic biliary and pancreatic drainage. In: Yamada T, editor. Text Book of Gastroenterology. Philadelphia, Pa, USA: J. B. Lippincott; 1995. pp. 2590–2617.
-
- Ferrucci JT, Jr., Mueller PR, Harbin WP. Percutaneous transhepatic biliary drainage. Technique, results, and applications. Radiology. 1980;135(1):1–13. - PubMed
-
- van Delden OM, Lameris JS. Percutaneous drainage and stenting for palliation of malignant bile duct obstruction. European Radiology. 2008;18:448–456. - PubMed
-
- Smith AC, Dowsett JF, Russell RCG, Hatfield ARW, Cotton PB. Randomised trial of endoscopic stenting versus surgical bypass in malignant low bileduct obstruction. Lancet. 1994;344(8938):1655–1660. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
