

Gaining a better understanding of respiratory health inequalities among cities: an ecological case study on elderly males in the larger French cities
- PMID: 23575258
- PMCID: PMC3735046
- DOI: 10.1186/1476-072X-12-19
Gaining a better understanding of respiratory health inequalities among cities: an ecological case study on elderly males in the larger French cities
Abstract
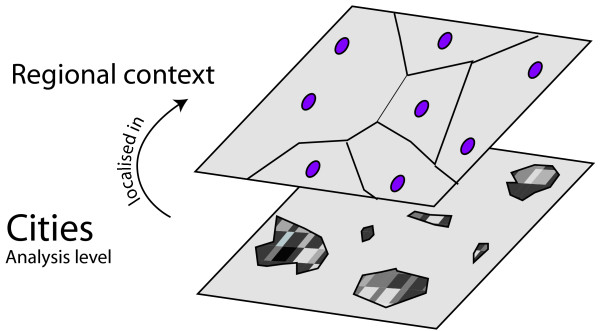
Background: In recent years, there have been a growing number of studies on spatial inequalities in health covering a variety of scales, from small areas to metropolitan areas or regions, and for various health outcomes. However, few investigations have compared health status between cities with a view to gaining a better understanding of the relationships between such inequalities and the social, economic and physical characteristics. This paper focuses on disparities in respiratory health among the 55 largest French cities. The aim is to explore the relationships between inter-urban health patterns, city characteristics and regional context, and to determine how far a city's health status relates to the features observed on different geographical scales.
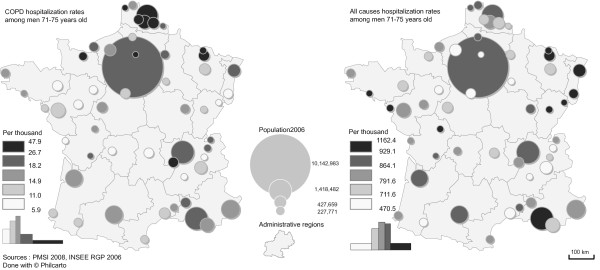
Methods: We used health data describing hospitalizations for Chronic Obstructive Pulmonary Disease (COPD) as a proxy for respiratory health, and the total number of hospitalizations (overall) as a proxy for general health. This last indicator was used as a benchmark. A large set of indicators relating to socioeconomic, physical and amenity aspects of the cities (urban units) was also constructed. Data were analyzed using linear correlations and multiple linear regression models.
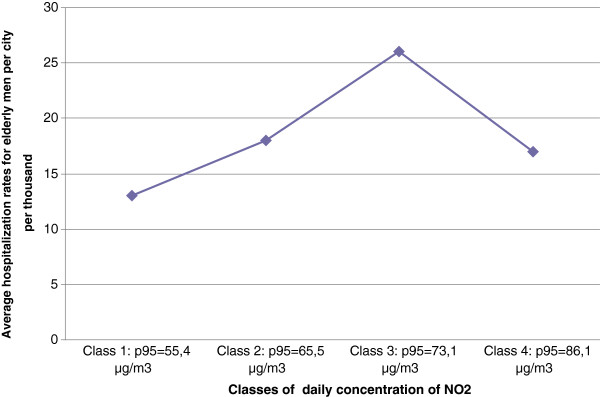
Results: The results suggest that socioeconomic characteristics are major discriminators for inequalities in respiratory health status among urban units. Indeed, once combined to socioeconomic characteristics, only a climate indicator remained significant among the physical indicators. It appeared that the pollution indicators which were significantly correlated with COPD hospitalization rates loosed significance when associated to the socio-economic indicators in a multiple regression. The analysis showed that among the socio-economic indicators, an employment indicator derived at the regional scale, and two indicators reflecting the unequal intra-urban spatial distribution of population according to their education, were the most efficient to describe differences in the respiratory health status of urban units.
Conclusion: In order to design effective urban policies, it is essential to gain a better understanding of the differences among cities in their entirety, rather than solely differences across small urban areas or individuals.
Contexte: Un nombre croissant d’études sur les inégalités spatiales de santé, conduites à des échelons très différents, des quartiers aux aires métropolitaines ou aux régions a été publié au cours des années récentes. Ces études couvrent des pathologies variées. Peu d’études ont cependant adopté une approche comparative et ont eu pour ambition d’expliquer les différences interurbaines de santé en mobilisant à la fois des indicateurs sociaux, économiques et physiques. Cet article propose une étude de cas sur les disparités interurbaines de santé respiratoires parmi les 55 plus grandes villes françaises. L’objectif ici est d’explorer les relations entre les différenciations interurbaines de santé et les caractéristiques des villes, en tenant compte de ces caractéristiques à différents échelons (ville, région, quartier).
Méthodes: Nous avons mobilisé une information sur les hospitalisations pour Broncho Pneumopathie Chronique Obstructive (BPCO) pour approcher la situation respiratoire des villes et sur l’ensemble des hospitalisations pour approcher la situation de santé générale de ces mêmes villes. Un grand nombre d’indicateurs socio-économiques, d’indicateurs décrivant l’environnement physique et les équipements de soins ont été construits pour décrire les villes. L’information a été analysée en utilisant des régressions linéaires simples et multiples.
Résultats: Les résultats suggèrent que les caractéristiques socio-économiques sont des facteurs majeurs de différenciation entre les villes du point de vue des situations de santé. Combinées aux indicateurs socio-économiques, seul l’indicateur des températures de janvier reste significatif. Les indicateurs de pollution, qui sont significativement associés aux taux d’hospitalisation pour BPCO, perdent de leur pouvoir explicatif lorsqu’ils sont associés aux indicateurs socio-économiques dans la régression multiple. Les résultats montrent que parmi les indicateurs économiques, le niveau de chômage régional s’associe à des indicateurs reflétant l’inégale répartition des populations, selon leur niveau d’éducation, à l’intérieur de la ville pour décrire de manière efficace les différences interurbaines de santé respiratoire.
Conclusion: Afin de mieux réfléchir aux politiques de santé, il paraît important de s’intéresser aussi aux aspects collectifs des différences interurbaines de santé et pas uniquement aux différences entre individus.
Figures


References
-
- Berry BJ. Cities as systems within systems of cities. Pap Reg Sci. 1964;13:147–163.
-
- Cummins S, Curtis S, Diez-Roux AV, Macintyre S. Understanding and representing “place” in health research: A relational approach. Soc Sci Med. 2007;65:1825–1838. - PubMed
-
- World Health Organization. World Health Statistics 2008. Geneva: World Health Organization; 2008. p. 112.
-
- Andersen ZJ, Hvidberg M, Jensen SS, Ketzel M, Loft S, Sorensen M, Tjonneland A, Overvad K, Raaschou-Nielsen O. Chronic obstructive pulmonary disease and long-term exposure to traffic-related Air pollution: a cohort study. Am J Respir Crit Care Med. 2010;183:455–461. - PubMed
-
- Atkinson RW, Ross Anderson H, Sunyer J, Ayres J, Baccini M, Vonk JM, Boumghar A, Forastiere F, Forsberg B, Touloumi G, Schwartz J, Katsouyanni K. Acute effects of particulate Air pollution on respiratory admissions results from APHEA 2 project. Am J Respir Crit Care Med. 2001;164:1860–1866. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
