

Ketamine pharmacology: an update (pharmacodynamics and molecular aspects, recent findings)
- PMID: 23575437
- PMCID: PMC6493357
- DOI: 10.1111/cns.12099
Ketamine pharmacology: an update (pharmacodynamics and molecular aspects, recent findings)
Abstract
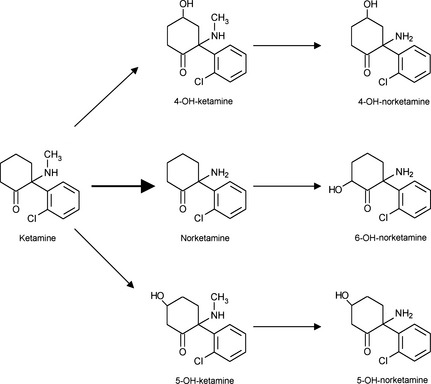
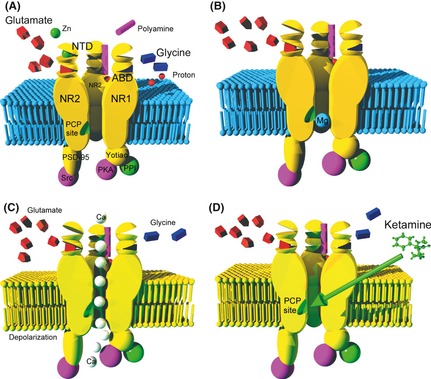
For more than 50 years, ketamine has proven to be a safe anesthetic drug with potent analgesic properties. The active enantiomer is S(+)-ketamine. Ketamine is mostly metabolized in norketamine, an active metabolite. During "dissociative anesthesia", sensory inputs may reach cortical receiving areas, but fail to be perceived in some association areas. Ketamine also enhances the descending inhibiting serotoninergic pathway and exerts antidepressive effects. Analgesic effects persist for plasma concentrations ten times lower than hypnotic concentrations. Activation of the (N-Methyl-D-Aspartate [NMDA]) receptor plays a fundamental role in long-term potentiation but also in hyperalgesia and opioid-induced hyperalgesia. The antagonism of NMDA receptor is responsible for ketamine's more specific properties. Ketamine decreases the "wind up" phenomenon, and the antagonism is more important if the NMDA channel has been previously opened by the glutamate binding ("use dependence"). Experimentally, ketamine may promote neuronal apoptotic lesions but, in usual clinical practice, it does not induce neurotoxicity. The consequences of high doses, repeatedly administered, are not known. Cognitive disturbances are frequent in chronic users of ketamine, as well as frontal white matter abnormalities. Animal studies suggest that neurodegeneration is a potential long-term risk of anesthetics in neonatal and young pediatric patients.
© 2013 John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Johnstone M, Evans V, Baigel S. Sernyl (CI‐395) in clinical anaesthesia. Br J Anaesth 1959;31:433–439. - PubMed
-
- Corssen G, Domino EF. Dissociative anesthesia: Further pharmacologic studies and first clinical experience with the phencyclidine derivative CI‐581. Anesth Analg 1966;45:29–40. - PubMed
-
- Domino EF, Chodoff P, Corssen G. Pharmacologic effects of CI‐581, a new dissociative anesthetic, in man. Clin Pharmacol Ther 1965;6:279–291. - PubMed
-
- Dayton PG, Stiller RL, Cook DR, Perel JM. The binding of ketamine to plasma proteins: Emphasis on human plasma. Eur J Clin Pharmacol 1983;24:825–831. - PubMed
-
- Schuttler J, Stanski DR, White PF, et al. Pharmacodynamic modeling of the EEG effects of ketamine and its enantiomers in man. J Pharmacokinet Biopharm 1987;15:241–253. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
