

Th1-Th17 cells contribute to the development of uropathogenic Escherichia coli-induced chronic pelvic pain
- PMID: 23577183
- PMCID: PMC3618515
- DOI: 10.1371/journal.pone.0060987
Th1-Th17 cells contribute to the development of uropathogenic Escherichia coli-induced chronic pelvic pain
Abstract
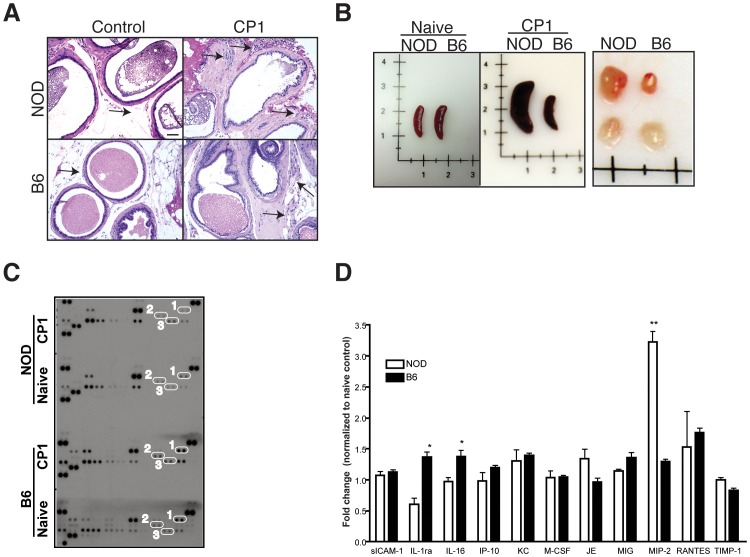
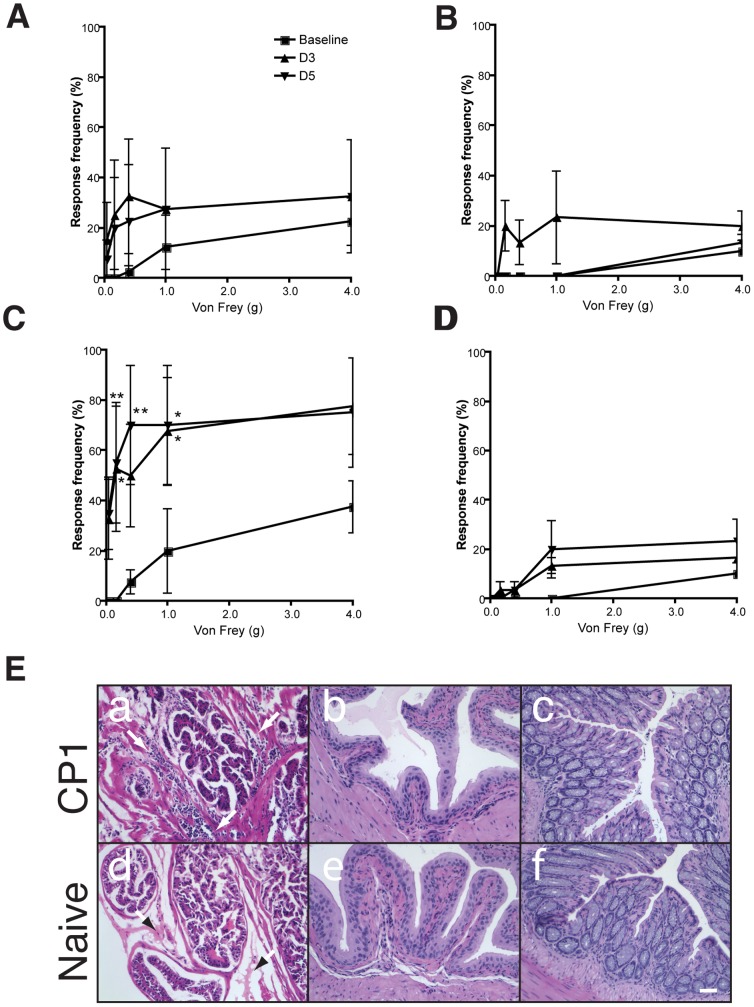
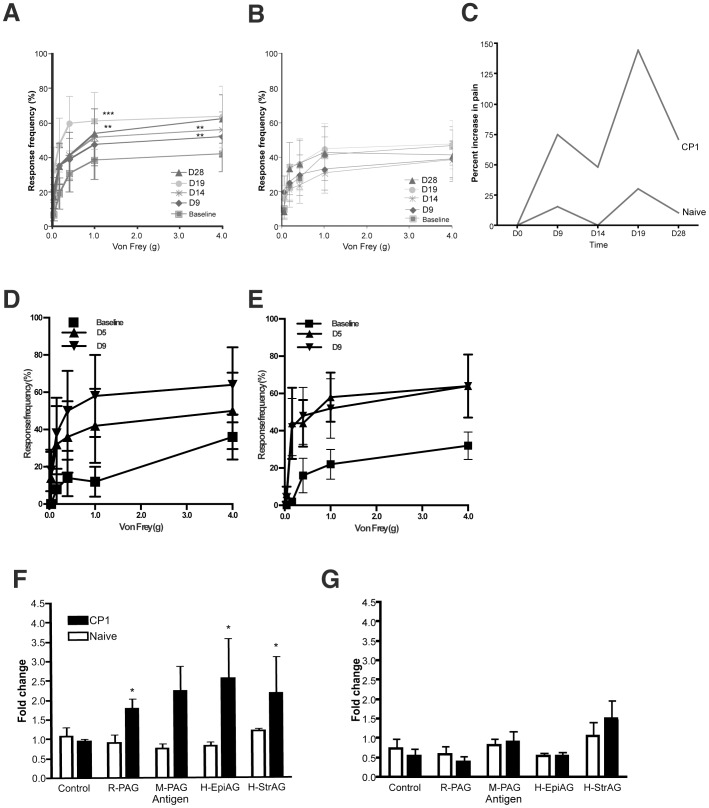
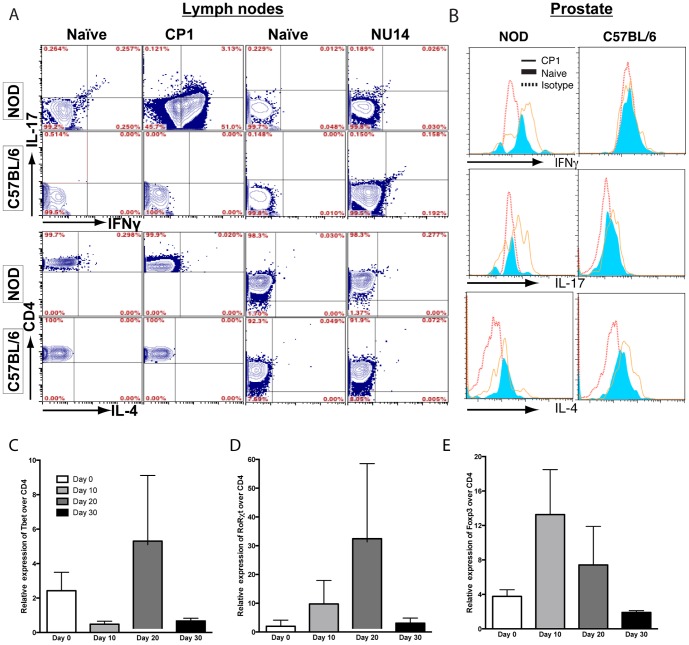
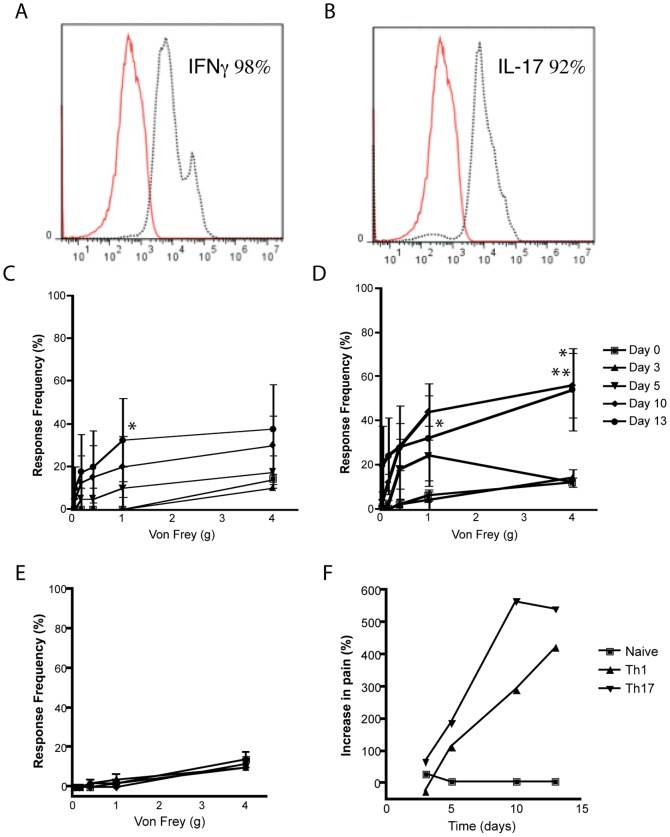
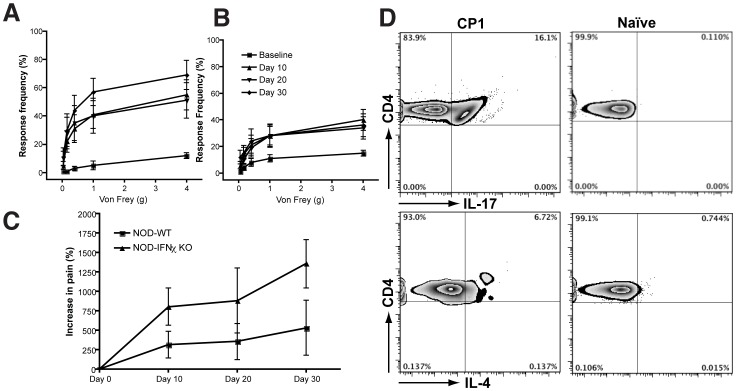
The etiology of chronic prostatitis/chronic pelvic pain syndrome in men is unknown but may involve microbes and autoimmune mechanisms. We developed an infection model of chronic pelvic pain in NOD/ShiLtJ (NOD) mice with a clinical Escherichia coli isolate (CP-1) from a patient with chronic pelvic pain. We investigated pain mechanisms in NOD mice and compared it to C57BL/6 (B6) mice, a strain resistant to CP-1-induced pain. Adoptive transfer of CD4+ T cells, but not serum, from CP-1-infected NOD mice was sufficient to induce chronic pelvic pain. CD4+ T cells in CP-1-infected NOD mice expressed IFN-γ and IL-17A but not IL-4, consistent with a Th1/Th17 immune signature. Adoptive transfer of ex-vivo expanded IFN-γ or IL-17A-expressing cells was sufficient to induce pelvic pain in naïve NOD recipients. Pelvic pain was not abolished in NOD-IFN-γ-KO mice but was associated with an enhanced IL-17A immune response to CP1 infection. These findings demonstrate a novel role for Th1 and Th17-mediated adaptive immune mechanisms in chronic pelvic pain.
Conflict of interest statement
Figures
Comment in
-
Re: Th1-Th17 cells contribute to the development of uropathogenic Escherichia coli-induced chronic pelvic pain.J Urol. 2014 Jun;191(6):1808-9. doi: 10.1016/j.juro.2014.03.029. Epub 2014 Mar 18. J Urol. 2014. PMID: 25280287 No abstract available.
References
-
- Collins MM, Stafford RS, O'Leary MP, Barry MJ (1998) How common is prostatitis? A national survey of physician visits. J Urol 159: 1224–1228. - PubMed
-
- Hua VN, Schaeffer AJ (2004) Acute and chronic prostatitis. Med Clin North Am 88: 483–494. - PubMed
-
- Nickel JC, Alexander RB, Schaeffer AJ, Landis JR, Knauss JS, et al. (2003) Leukocytes and bacteria in men with chronic prostatitis/chronic pelvic pain syndrome compared to asymptomatic controls. J Urol 170: 818–822. - PubMed
-
- Leskinen MJ, Rantakokko-Jalava K, Manninen R, Leppilahti M, Marttila T, et al. (2003) Negative bacterial polymerase chain reaction (PCR) findings in prostate tissue from patients with symptoms of chronic pelvic pain syndrome (CPPS) and localized prostate cancer. Prostate 55: 105–110. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
