

Radiographically occult and subtle fractures: a pictorial review
- PMID: 23577253
- PMCID: PMC3613077
- DOI: 10.1155/2013/370169
Radiographically occult and subtle fractures: a pictorial review
Abstract
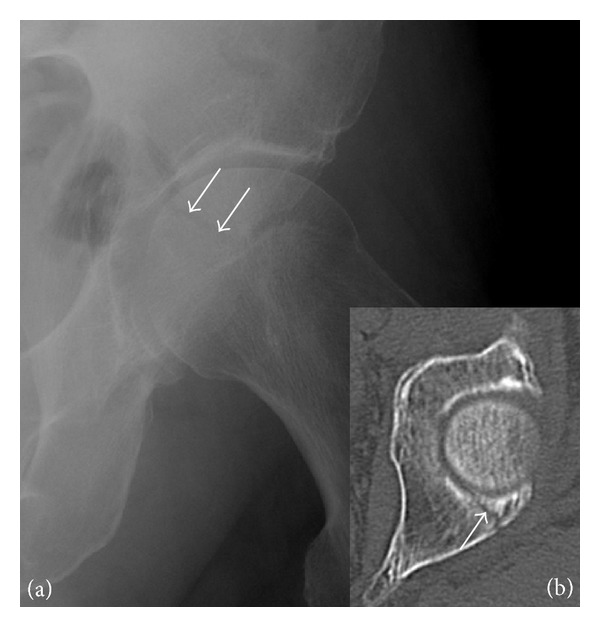
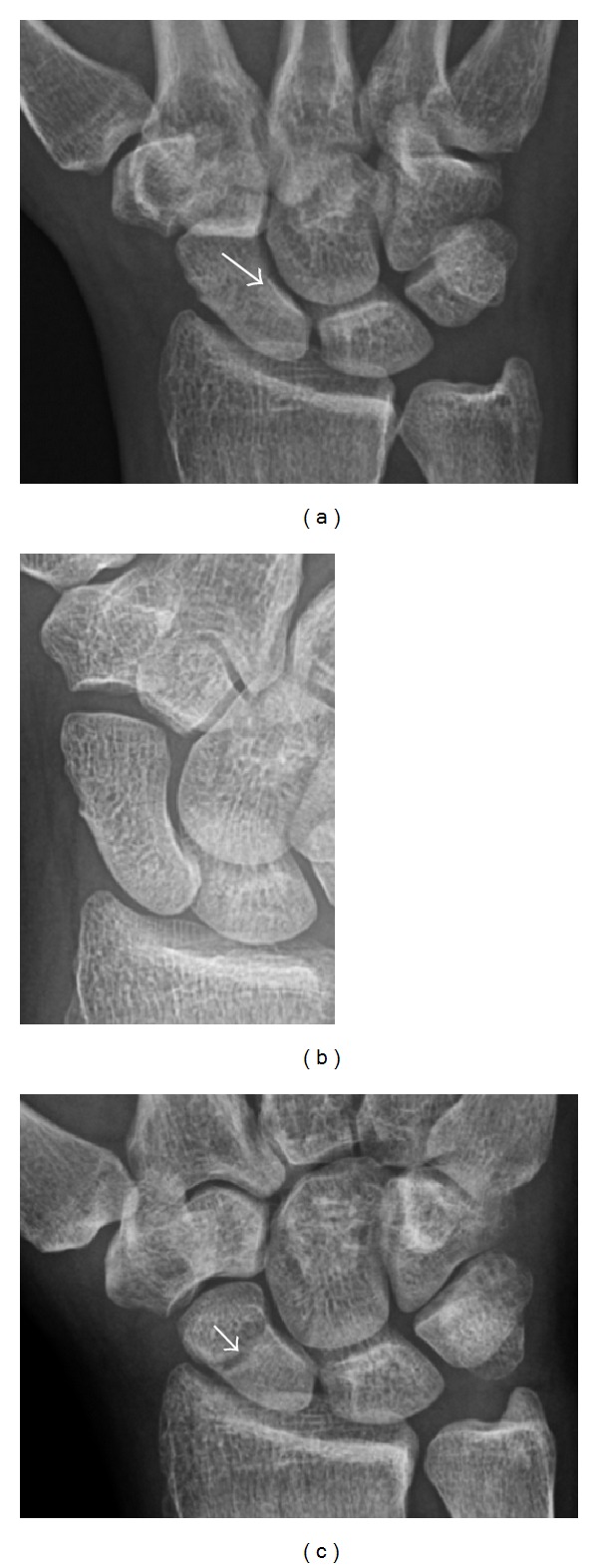
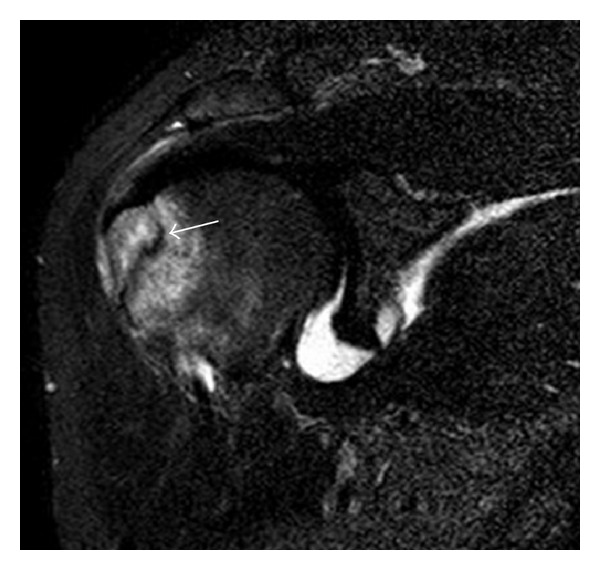
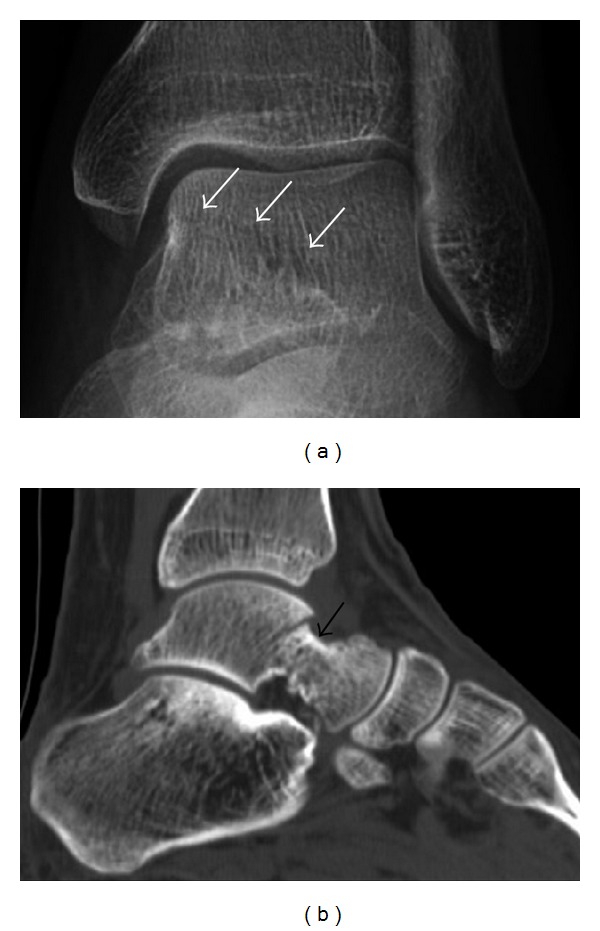
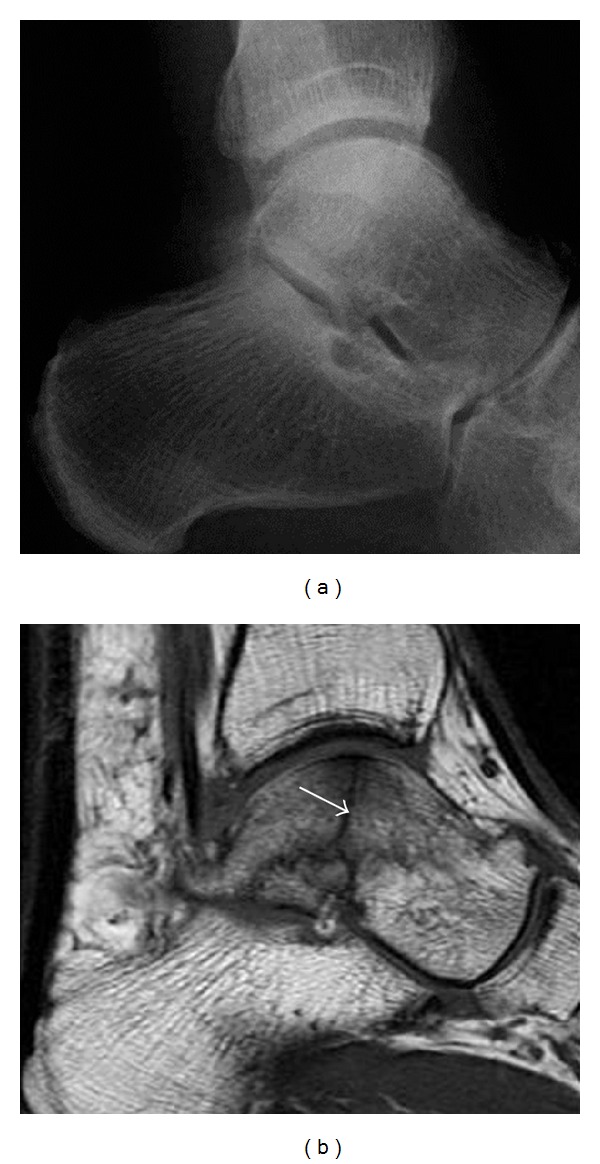
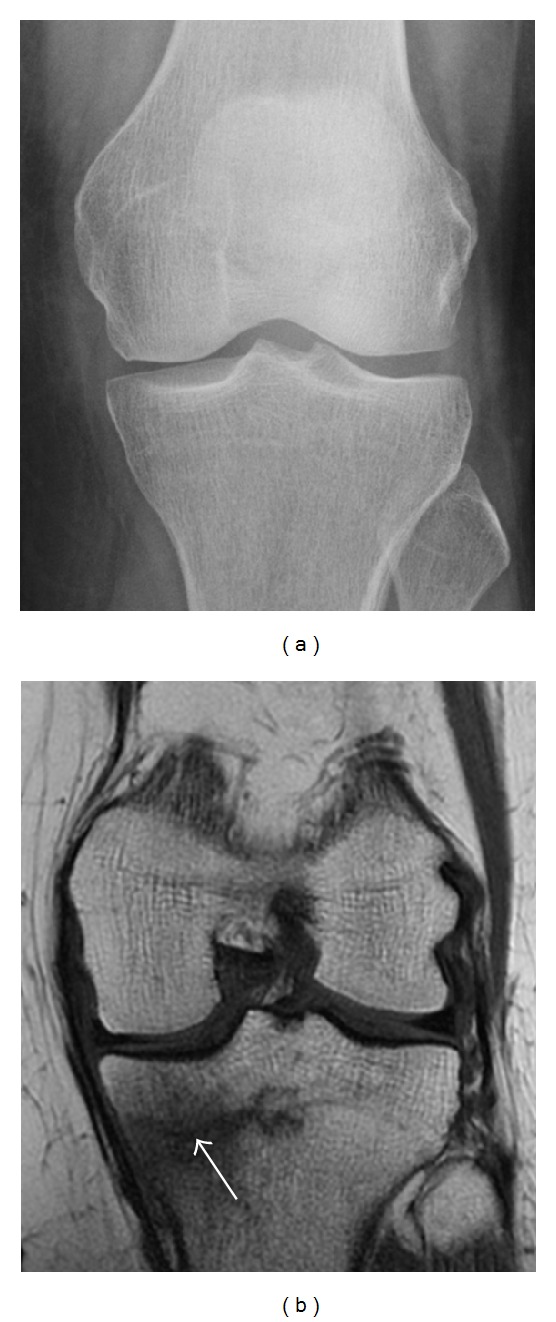
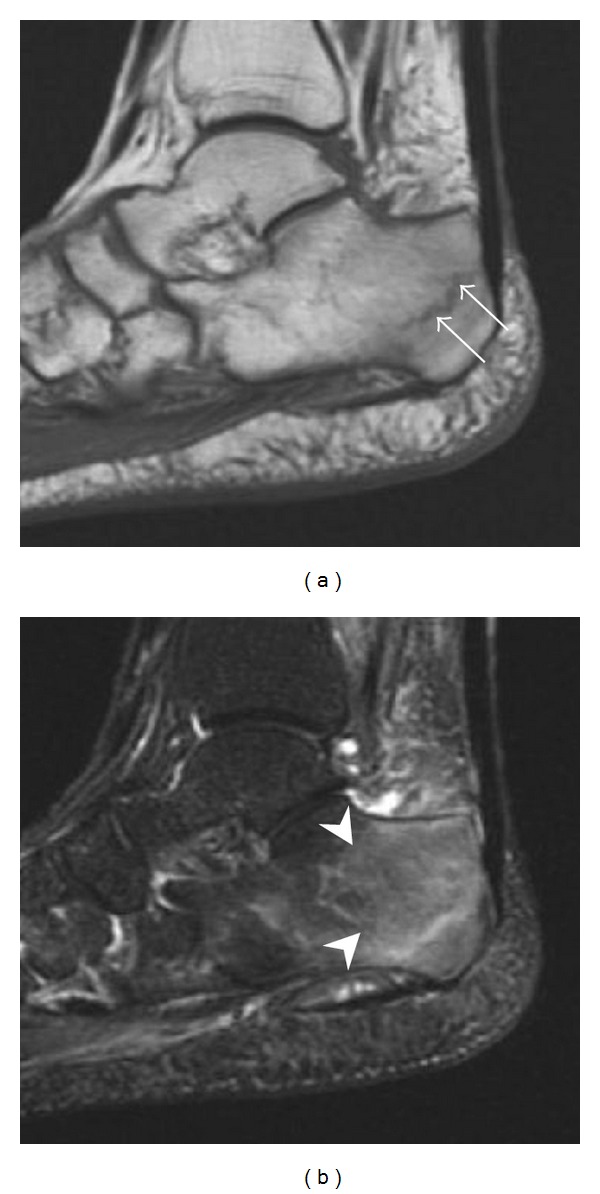
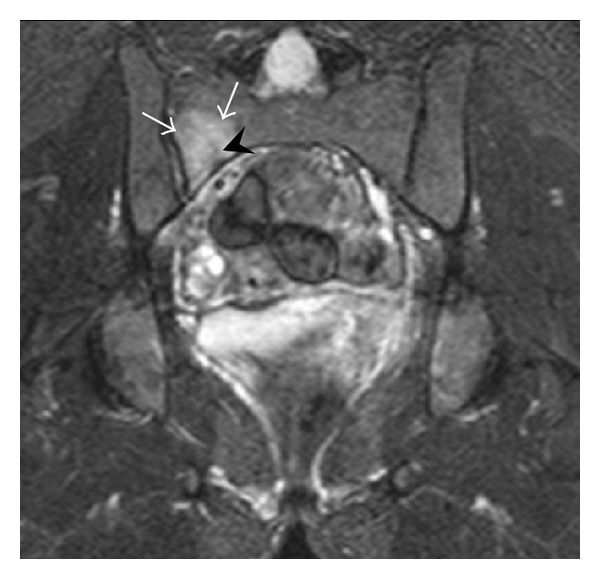
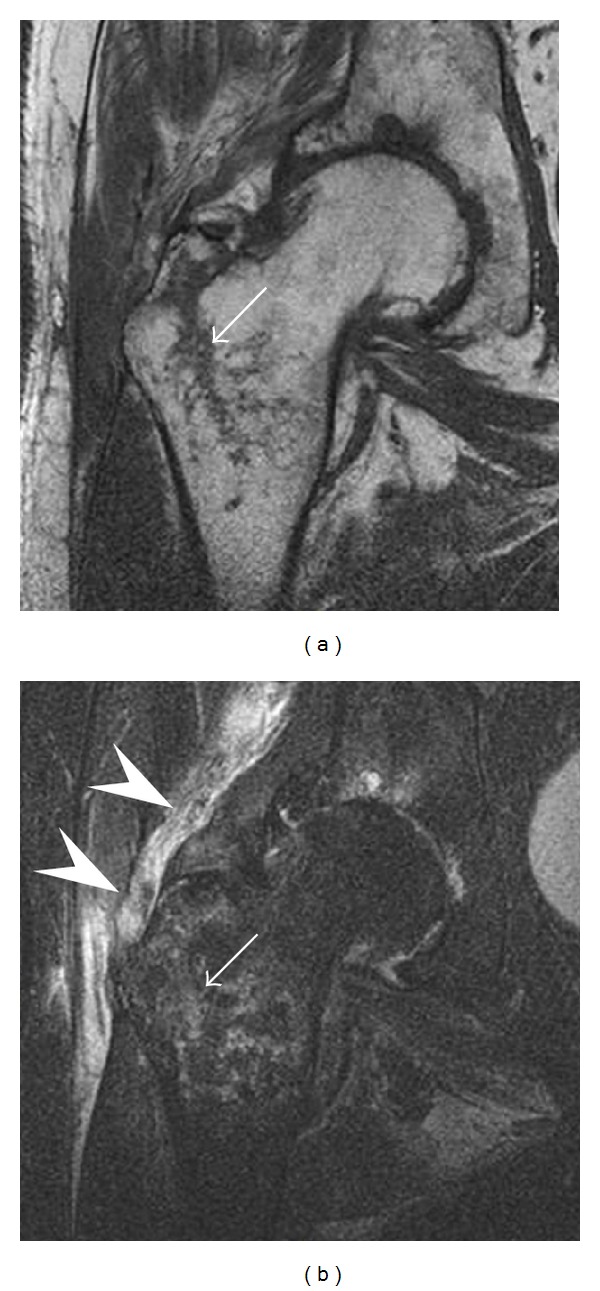
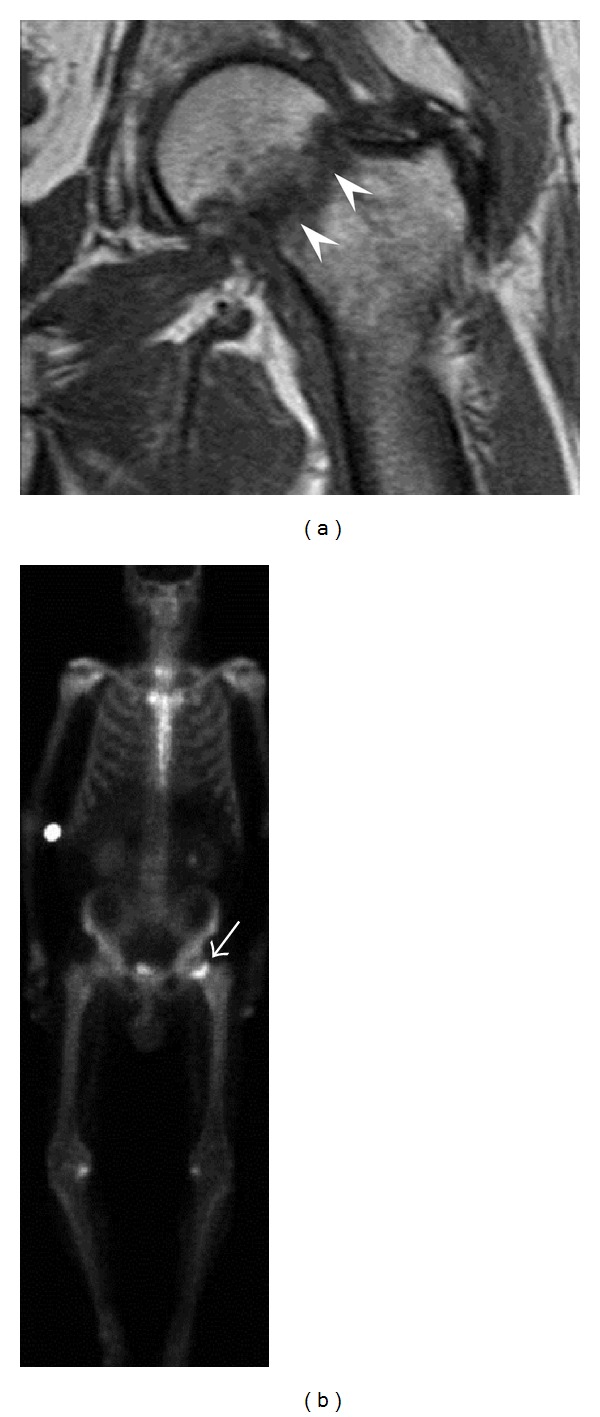
Radiographically occult and subtle fractures are a diagnostic challenge. They may be divided into (1) "high energy trauma fracture," (2) "fatigue fracture" from cyclical and sustained mechanical stress, and (3) "insufficiency fracture" occurring in weakened bone (e.g., in osteoporosis and postradiotherapy). Independently of the cause, the initial radiographic examination can be negative either because the findings seem normal or are too subtle. Early detection of these fractures is crucial to explain the patient's symptoms and prevent further complications. Advanced imaging tools such as computed tomography, magnetic resonance imaging, and scintigraphy are highly valuable in this context. Our aim is to raise the awareness of radiologists and clinicians in these cases by presenting illustrative cases and a discussion of the relevant literature.
Figures




References
-
- Sshwartz DT. ACEP Scientific Assembly. Boston Convention and Exhibition Center; 2009. Ten most coommonly missed radiographic findings in the ED.
-
- Goldfarb CA, Yin Y, Gilula LA, Fisher AJ, Boyer MI. Wrist fractures: what the clinician wants to know. Radiology. 2001;219(1):11–28. - PubMed
-
- Pentecost RL, Murray RA, Brindley HH. Fatigue, insufficiency, and pathologic fractures. The Journal of the American Medical Association. 1964;187:1001–1004. - PubMed
-
- Fayad LM, Kamel IR, Kawamoto S, Bluemke DA, Frassica FJ, Fishman EK. Distinguishing stress fractures from pathologic fractures: a multimodality approach. Skeletal Radiology. 2005;34(5):245–259. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
