Selective shunt during carotid endarterectomy using routine awake test with respect to a lower shunt rate
- PMID: 23577319
- PMCID: PMC3616278
- DOI: 10.4174/jkss.2013.84.4.238
Selective shunt during carotid endarterectomy using routine awake test with respect to a lower shunt rate
Abstract
Purpose: To evaluate shunt rate and discuss the resultsrelated to selective shunt placement during carotid endarterectomy (CEA) using routine awake test.
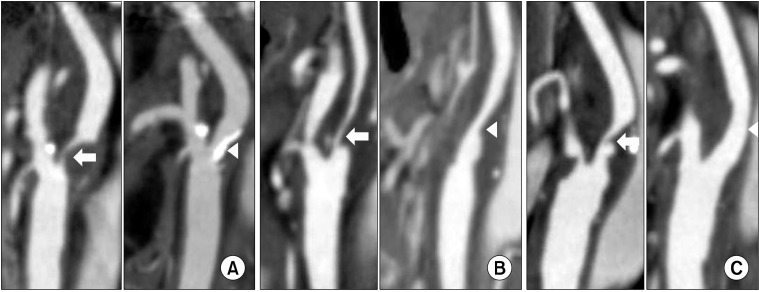
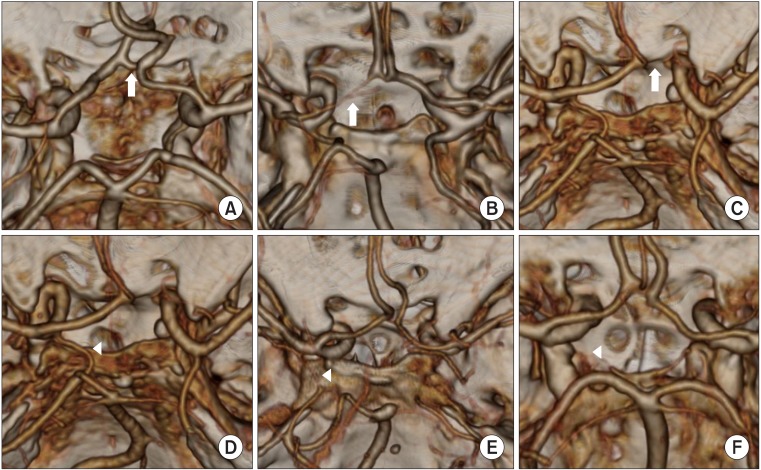
Methods: Patients with CEA from 2007 to 2011 were retrospectively reviewed from prospectively collected data. The need for shunt placement was determined by the awake test, based on the alteration in the neurologic examination. We collected data by using the clinical records and imaging studies, and investigated factors related to selective shunt such as collateral circulation and contralateral internal carotid artery (ICA) stenosis.
Results: There were 45 CEAs under regional anesthesia with the awake test in 44 patients. The mean age was 61.8 ± 7.1 years old. There were 82.2% (37/45) of males, and 68.9% (31/45) of symptomatic patients. Selective shunt placement had been performed in only two (4.4%) patients. Among them fewer cases (4%) had severe (stenosis >70%) contralateral ICA lesions, and more cases (91%) of complete morphology of the anterior or posterior circulation in the circle of Willis. There was no perioperative stroke, myocardial infarctionor death, and asymptomatic new brain lesions were detected in 4 patients (9%), including 2 cases of selective shunt placement.
Conclusion: CEA under routine awake test could besafe and feasible method with low shunt placement rate in selected patients.
Keywords: Brain ischemia; Carotid endarterectomy; Intraoperative monitoring; Prevention.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991;325:445–453. - PubMed
-
- Frawley JE, Hicks RG, Gray LJ, Niesche JW. Carotid endarterectomy without a shunt for symptomatic lesions associated with contralateral severe stenosis or occlusion. J Vasc Surg. 1996;23:421–427. - PubMed
-
- Hertzer NR, O'Hara PJ, Mascha EJ, Krajewski LP, Sullivan TM, Beven EG. Early outcome assessment for 2228 consecutive carotid endarterectomy procedures: the Cleveland Clinic experience from 1989 to 1995. J Vasc Surg. 1997;26:1–10. - PubMed
-
- Lee KB, Lee KH, Chung CS, Kim GM, Byun HS, Jeon P, et al. Carotid endarterectomy: analysis of early complications (<30 days) and risk factors for postoperative new brain infarction. J Korean Surg Soc. 2009;77:195–201.
-
- Gumerlock MK, Neuwelt EA. Carotid endarterectomy: to shunt or not to shunt. Stroke. 1988;19:1485–1490. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous