

Echocardiographic methods, quality review, and measurement accuracy in a randomized multicenter clinical trial of Marfan syndrome
- PMID: 23582510
- PMCID: PMC3779059
- DOI: 10.1016/j.echo.2013.02.018
Echocardiographic methods, quality review, and measurement accuracy in a randomized multicenter clinical trial of Marfan syndrome
Abstract
Background: The Pediatric Heart Network is conducting a large international randomized trial to compare aortic root growth and other cardiovascular outcomes in 608 subjects with Marfan syndrome randomized to receive atenolol or losartan for 3 years. The authors report here the echocardiographic methods and baseline echocardiographic characteristics of the randomized subjects, describe the interobserver agreement of aortic measurements, and identify factors influencing agreement.
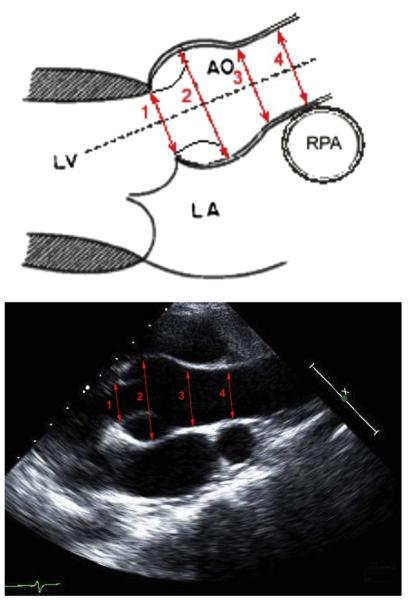
Methods: Individuals aged 6 months to 25 years who met the original Ghent criteria and had body surface area-adjusted maximum aortic root diameter (ROOTmax) Z scores > 3 were eligible for inclusion. The primary outcome measure for the trial is the change over time in ROOTmaxZ score. A detailed echocardiographic protocol was established and implemented across 22 centers, with an extensive training and quality review process.
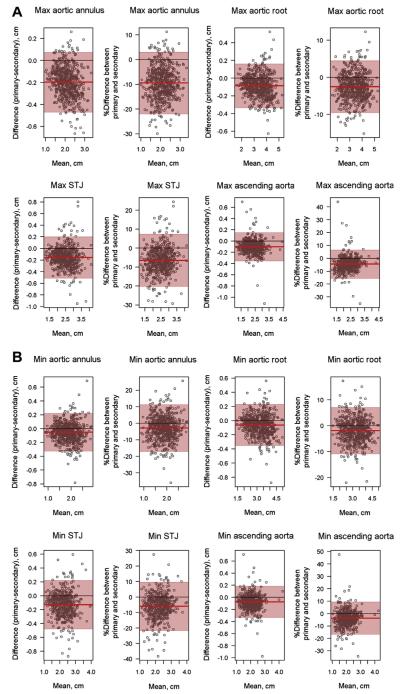
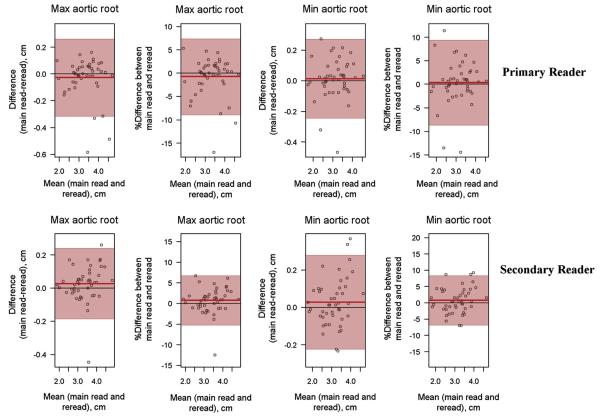
Results: Interobserver agreement for the aortic measurements was excellent, with intraclass correlation coefficients ranging from 0.921 to 0.989. Lower interobserver percentage error in ROOTmax measurements was independently associated (model R(2) = 0.15) with better image quality (P = .002) and later study reading date (P < .001). Echocardiographic characteristics of the randomized subjects did not differ by treatment arm. Subjects with ROOTmaxZ scores ≥ 4.5 (36%) were more likely to have mitral valve prolapse and dilation of the main pulmonary artery and left ventricle, but there were no differences in aortic regurgitation, aortic stiffness indices, mitral regurgitation, or left ventricular function compared with subjects with ROOTmaxZ scores < 4.5.
Conclusions: The echocardiographic methodology, training, and quality review process resulted in a robust evaluation of aortic root dimensions, with excellent reproducibility.
Copyright © 2013 American Society of Echocardiography. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- De Paepe A, Devereux RB, Dietz HC, Hennekam RC, Pyeritz RE. Revised diagnostic criteria for the Marfan syndrome. Am J Med Genet. 1996;62:417–26. - PubMed
-
- Haycock GB, Schwartz GJ, Wisotsky DH. Geometric method for measuring body surface area: a height-weight formula validated in infants, children, and adults. J Pediatr. 1978;93:62–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HL068288/HL/NHLBI NIH HHS/United States
- HL068285/HL/NHLBI NIH HHS/United States
- U01 HL068279/HL/NHLBI NIH HHS/United States
- U01 HL068290/HL/NHLBI NIH HHS/United States
- U10 HL068270/HL/NHLBI NIH HHS/United States
- U01 HL068281/HL/NHLBI NIH HHS/United States
- U01 HL085057/HL/NHLBI NIH HHS/United States
- HL068290/HL/NHLBI NIH HHS/United States
- U01 HL068269/HL/NHLBI NIH HHS/United States
- U10 HL109816/HL/NHLBI NIH HHS/United States
- HL068279/HL/NHLBI NIH HHS/United States
- U01 HL068288/HL/NHLBI NIH HHS/United States
- U01 HL068270/HL/NHLBI NIH HHS/United States
- HL085057/HL/NHLBI NIH HHS/United States
- HL068281/HL/NHLBI NIH HHS/United States
- U01 HL068292/HL/NHLBI NIH HHS/United States
- HL068269/HL/NHLBI NIH HHS/United States
- HL068270/HL/NHLBI NIH HHS/United States
- U01 HL068285/HL/NHLBI NIH HHS/United States
- HL068292/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
