

Predictors of electrocerebral inactivity with deep hypothermia
- PMID: 23582829
- PMCID: PMC3800484
- DOI: 10.1016/j.jtcvs.2013.03.022
Predictors of electrocerebral inactivity with deep hypothermia
Abstract
Objective: Cooling to electrocerebral inactivity (ECI) by electroencephalography (EEG) remains the gold standard to maximize cerebral and systemic organ protection during deep hypothermic circulatory arrest (DHCA). We sought to determine predictors of ECI to help guide cooling protocols when EEG monitoring is unavailable.
Methods: Between July 2005 and July 2011, 396 patients underwent thoracic aortic operation with DHCA; EEG monitoring was used in 325 (82%) of these patients to guide the cooling strategy, and constituted the study cohort. Electroencephalographic monitoring was used for all elective cases and, when available, for nonelective cases. Multivariable linear regression was used to assess predictors of the nasopharyngeal temperature and cooling time required to achieve ECI.
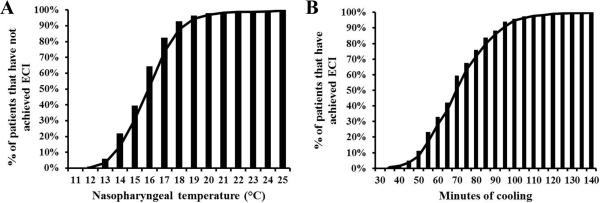
Results: Cooling to a nasopharyngeal temperature of 12.7°C or for a duration of 97 minutes was required to achieve ECI in >95% of patients. Only 7% and 11% of patients achieved ECI by 18°C or 50 minutes of cooling, respectively. No independent predictors of nasopharyngeal temperature at ECI were identified. Independent predictors of cooling time included body surface area (18 minutes/m(2)), white race (7 minutes), and starting nasopharyngeal temperature (3 minutes/°C). Low complication rates were observed (ischemic stroke, 1.5%; permanent paraparesis/paraplegia, 1.5%; new-onset dialysis, 2.2%; and 30-day/in-hospital mortality, 4.3%).
Conclusions: Cooling to a nasopharyngeal temperature of 12.7°C or for a duration of 97 minutes achieved ECI in >95% of patients in our study population. However, patient-specific factors were poorly predictive of the temperature or cooling time required to achieve ECI, necessitating EEG monitoring for precise ECI detection.
Copyright © 2014 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Michenfelder JD, Milde JH. The effect of profound levels of hypothermia (below 14 degrees C) on canine cerebral metabolism. J Cereb Blood Flow Metab. 1992 Sep;12(5):877–80. - PubMed
-
- Mezrow CK, Midulla PS, Sadeghi AM, Gandsas A, Wang W, Dapunt OE, et al. Evaluation of cerebral metabolism and quantitative electroencephalography after hypothermic circulatory arrest and low-flow cardiopulmonary bypass at different temperatures. J Thorac Cardiovasc Surg. 1994 Apr;107(4):1006–19. - PubMed
-
- Weiss AJ, Lin HM, Bischoff MS, Scheumann J, Lazala R, Griepp RB, et al. A propensity score-matched comparison of deep versus mild hypothermia during thoracoabdominal aortic surgery. J Thorac Cardiovasc Surg. 2012 Jan;143(1):186–93. - PubMed
-
- Stecker MM, Cheung AT, Pochettino A, Kent GP, Patterson T, Weiss SJ, et al. Deep hypothermic circulatory arrest: I. Effects of cooling on electroencephalogram and evoked potentials. Ann Thorac Surg. 2001 Jan;71(1):14–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
