

Primary fascial closure versus staged closure with silo in patients with gastroschisis: a meta-analysis
- PMID: 23583145
- PMCID: PMC4103994
- DOI: 10.1016/j.jpedsurg.2013.01.020
Primary fascial closure versus staged closure with silo in patients with gastroschisis: a meta-analysis
Abstract
Background/purpose: Gastroschisis is the most common congenital abdominal wall defect. Despite advances in the surgical closure of gastroschisis, consensus is lacking as to which method results in the best patient outcomes. The purpose of this meta-analysis was to compare short-term outcomes associated with primary fascial closure and staged repair with a silo in patients with gastroschisis.
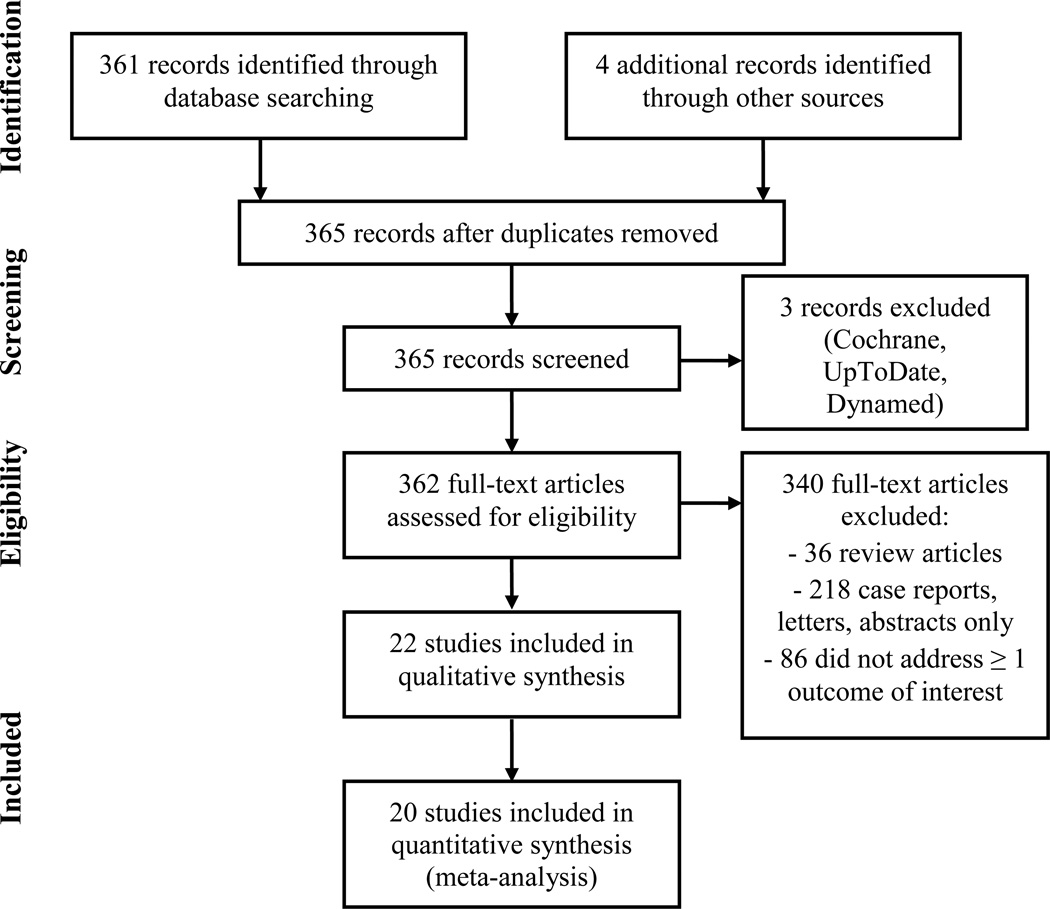
Methods: We reviewed Medline citations, as well as the Cochrane Database of Systematic Reviews, between January 1, 1996 and June 1, 2012. Articles were identified using the search term "gastroschisis" and [("treatment outcome" or "prognosis") or randomized controlled trials]. Case reports, reviews, letters, abstracts only, non-English abstracts, and studies that did not address at least one of the outcomes of interest were excluded from the meta-analysis. Two independent reviewers identified relevant articles for final inclusion. A standard data collection form created by the authors was used to extract study information, including study design, patient characteristics, and reported patient outcomes. The data were analyzed using standard meta-analytic techniques.
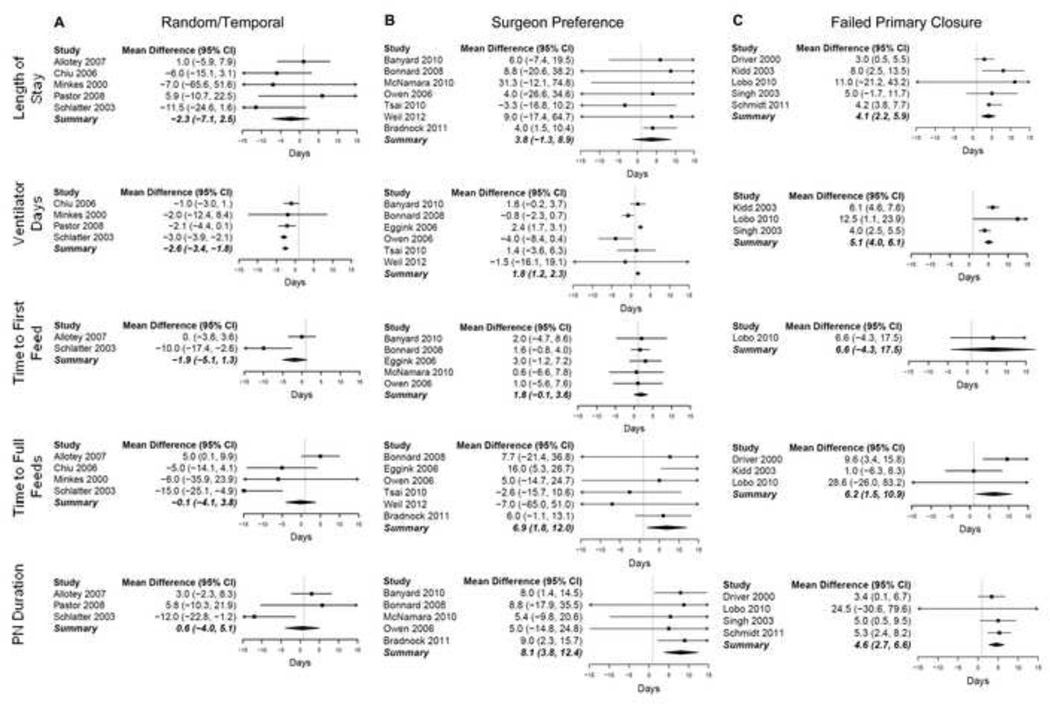
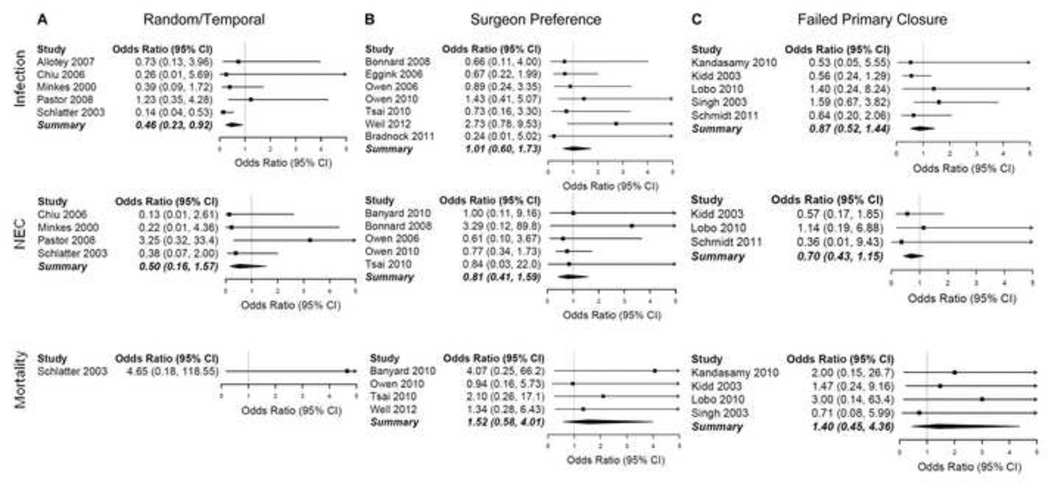
Results: Twenty studies were included in the meta-analysis. In the five studies that selected closure method randomly or as a temporal shift in practice, silo was associated with better outcomes, with a significant reduction in ventilator days (p<0.0001), time to first feed (p=0.04), and infection rates (p=0.03). When all studies were included, primary closure was associated with improved outcomes.
Conclusions: Silo closure is associated with better clinical outcomes in the studies with the least selection bias. Larger prospective studies are needed to definitively determine the best closure technique.
Copyright © 2013 Elsevier Inc. All rights reserved.
Conflict of interest statement
There are no conflicts of interest to disclose.
Figures
References
-
- Mortellaro VE, St Peter SD, Fike FB, et al. Review of the evidence on the closure of abdominal wall defects. Pediatr Surg Int. 2011;27(4):391–397. - PubMed
-
- Holland AJ, Walker K, Badawi N. Gastroschisis: An update. Pediatr Surg Int. 2010;26(9):871–878. - PubMed
-
- Abdullah F, Arnold MA, Nabaweesi R, et al. Gastroschisis in the united states 1988–2003: Analysis and risk categorization of 4344 patients. J Perinatol. 2007;27(1):50–55. - PubMed
-
- Fillingham A, Rankin J. Prevalence, prenatal diagnosis and survival of gastroschisis. Prenat Diagn. 2008;28(13):1232–1237. - PubMed
-
- Marven S, Owen A. Contemporary postnatal surgical management strategies for congenital abdominal wall defects. Semin Pediatr Surg. 2008;17(4):222–235. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
