

Management of gastric polyps: an endoscopy-based approach
- PMID: 23583466
- PMCID: PMC3962745
- DOI: 10.1016/j.cgh.2013.03.019
Management of gastric polyps: an endoscopy-based approach
Abstract
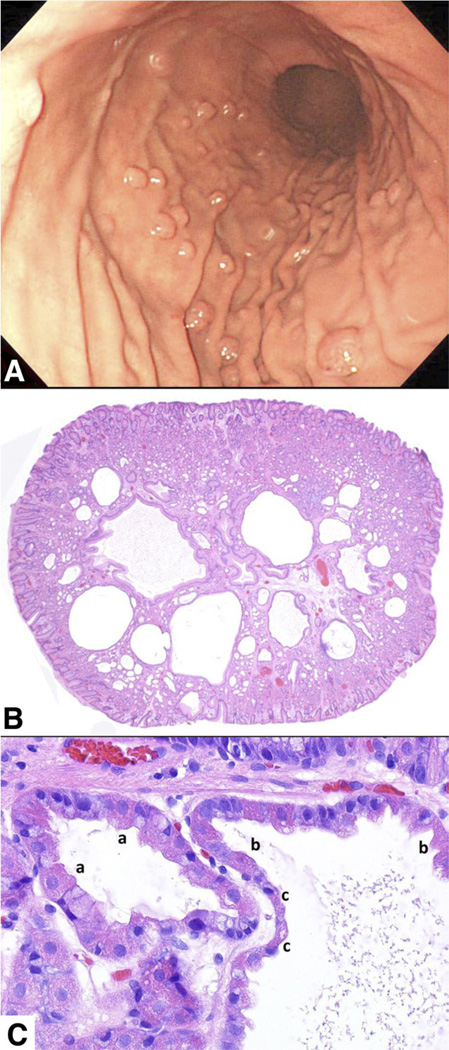
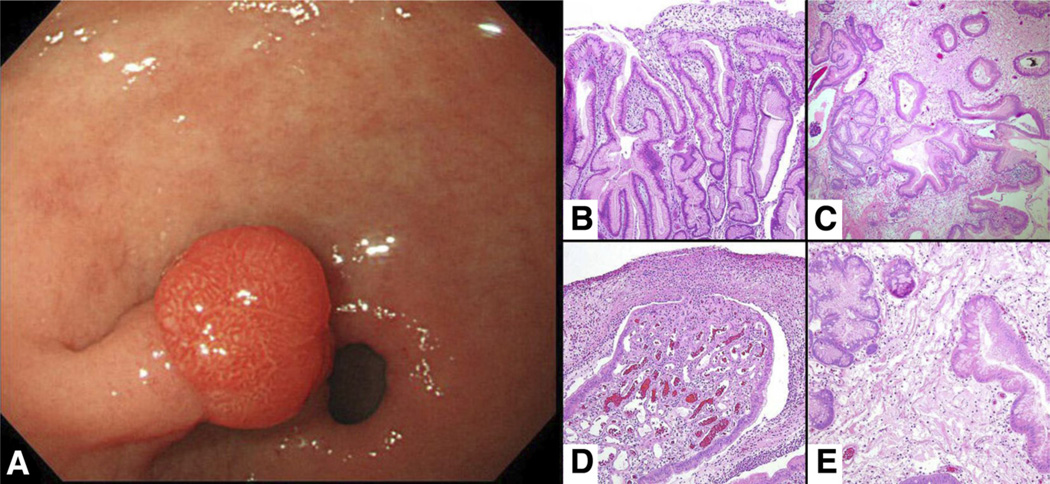
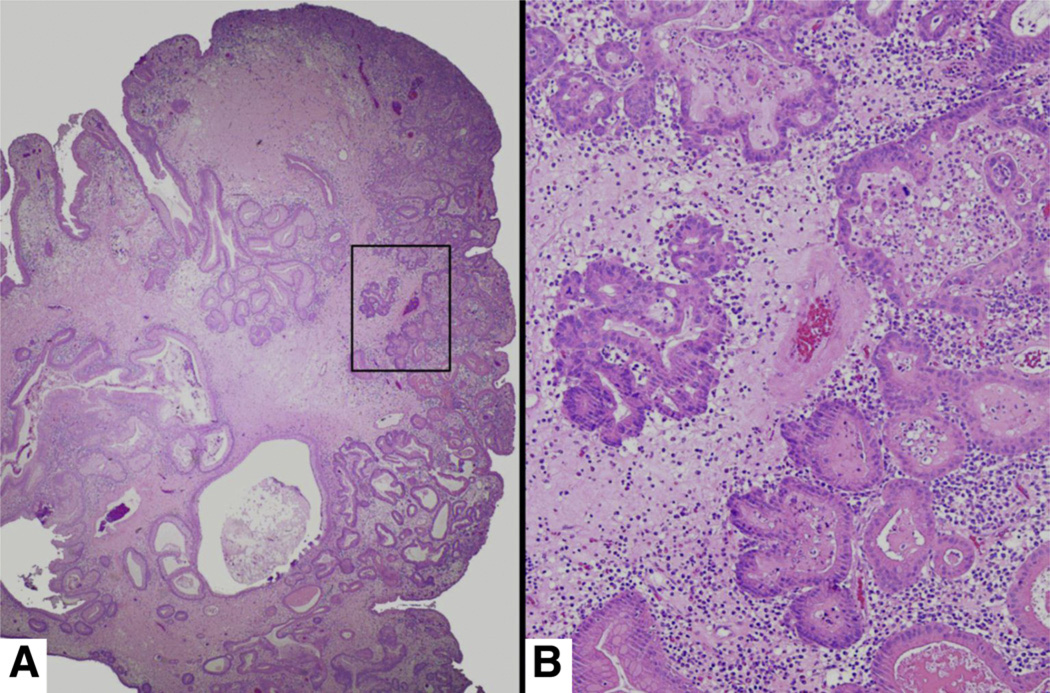
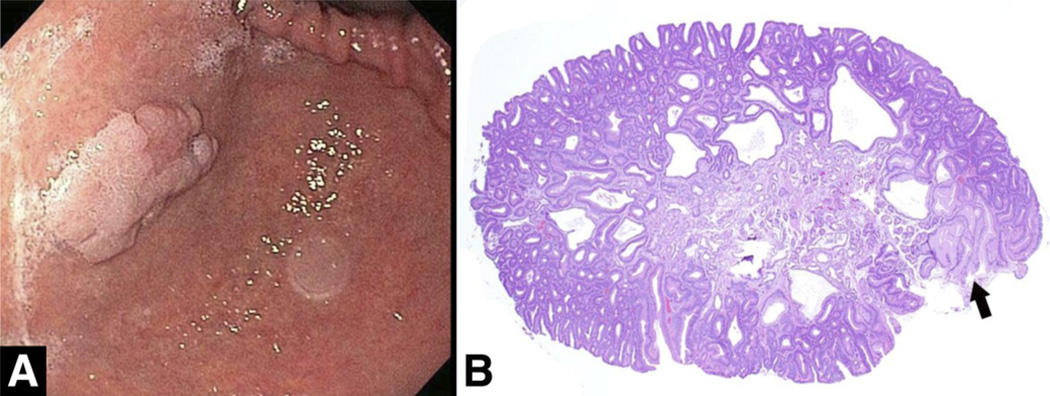
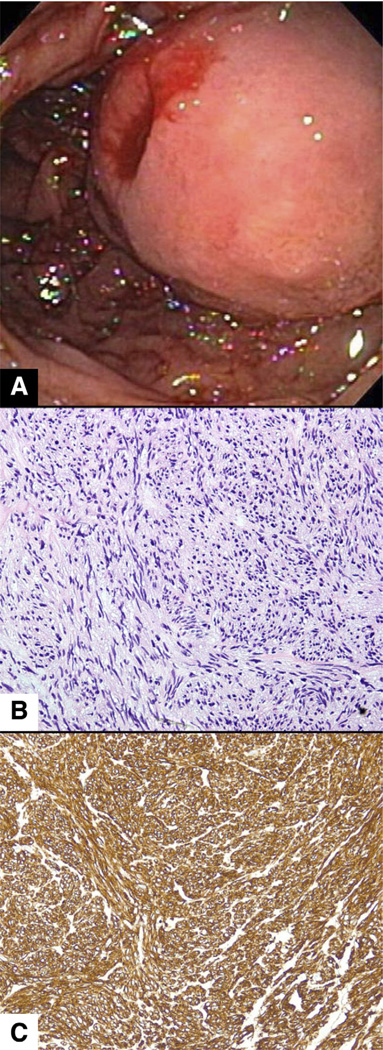
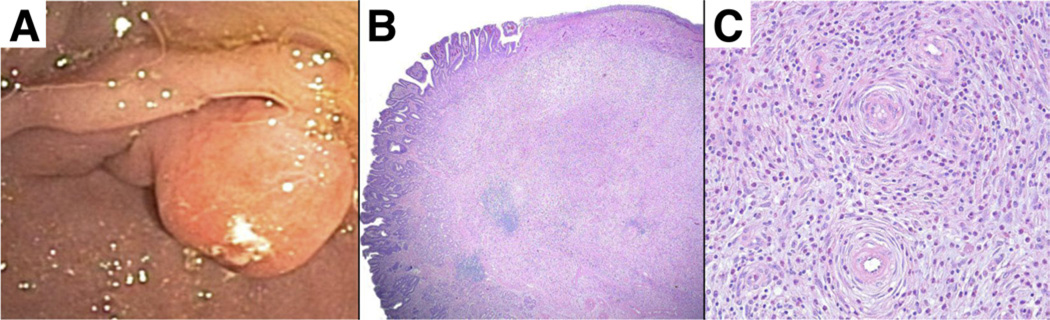
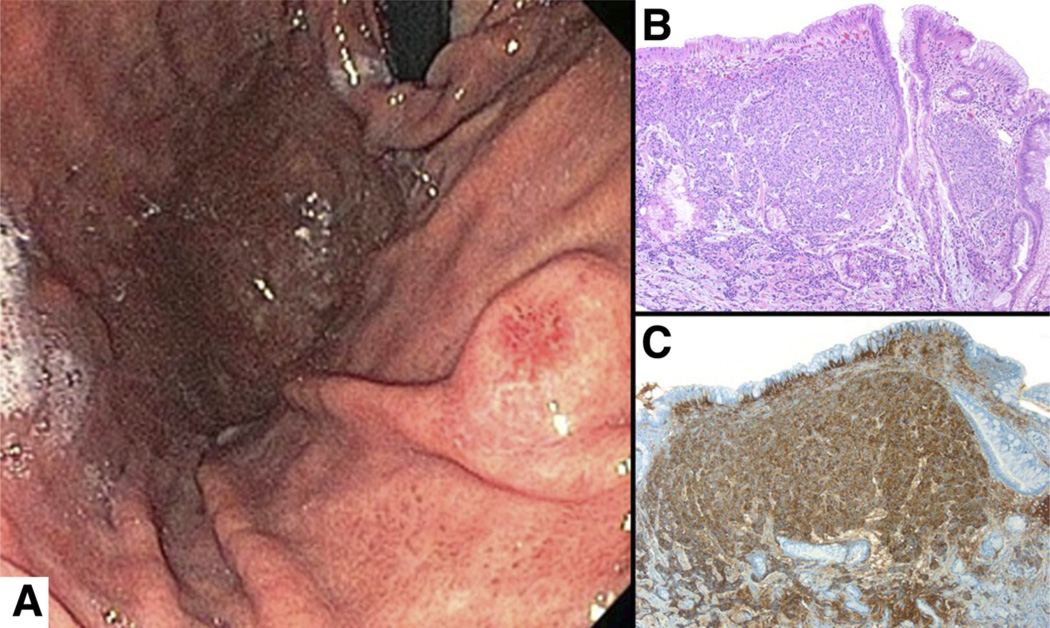
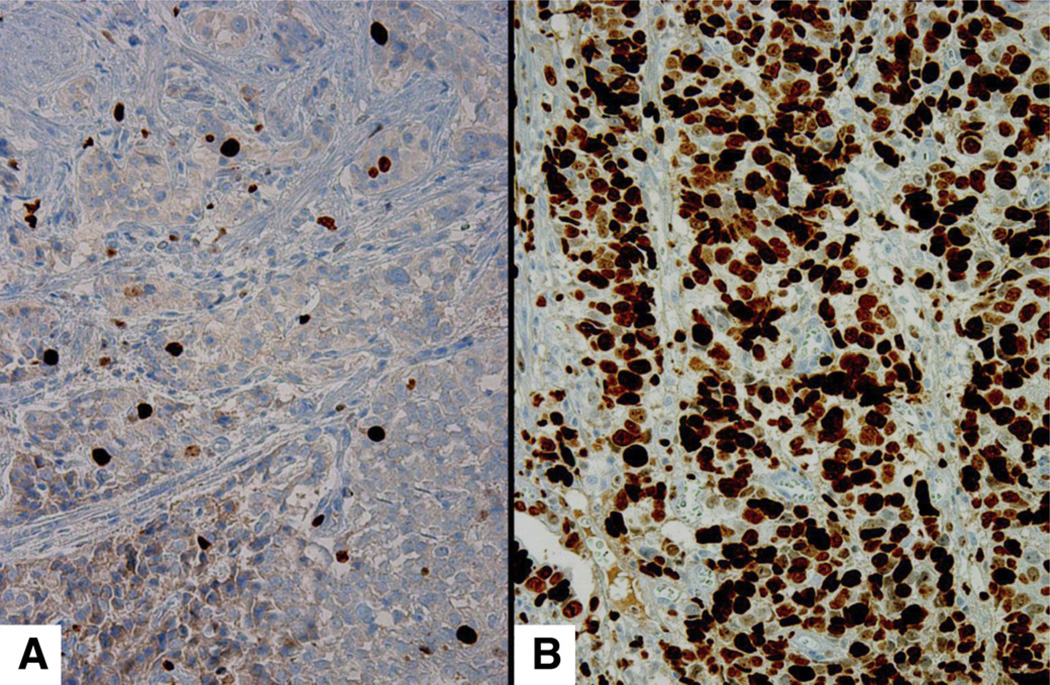
The endoscopic finding of a gastric polyp and the histopathologic report that follows may leave clinicians with questions that have not been addressed in formal guidelines: do all polyps need to be excised, or can they just be sampled for biopsy? If so, which ones and how many should be sampled? What follow-up evaluation is needed, if any? This review relies on the existing literature and our collective experience to provide practical answers to these questions. Fundic gland polyps, now the most frequent gastric polyps in Western countries because of widespread use of proton pump inhibitors, and hyperplastic polyps, the second most common polyps notable for their association with gastritis and their low but important potential for harboring dysplastic or neoplastic foci, are discussed in greater detail. Adenomas have had their name changed to raised intraepithelial neoplasia and are decreasing in parallel with Helicobacter pylori infection; however, they do retain their importance as harbingers of gastric cancer, particularly in East Asia. Gastrointestinal stromal tumors have low incidence and no known associations, but their malignant potential is high; early diagnosis and proper management are crucial. Although rare and benign, inflammatory fibroid polyps need to recognized, particularly by pathologists, to avoid misdiagnosis. Gastric neuroendocrine tumors (carcinoids) are important because of their association with either atrophic gastritis or the multiple endocrine neoplasia syndromes; those that do not arise in these backgrounds have high malignant potential and require aggressive management. The review concludes with some practical suggestions on how to approach gastric polyps detected at endoscopy.
Keywords: ECL; EGD; Endoscopic Management; GIST; Gastric Polyps; OLGA; Operative Link for Gastritis Assessment; PPI; enterochromaffin-like; esophagogastroduodenoscopy; gastrointestinal stromal tumors; proton pump inhibitor.
Copyright © 2013 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
The authors disclose no conflicts.
Figures
References
-
- Carmack SW, Genta RM, Schuler CM, et al. The current spectrum of gastric polyps: a 1-year national study of over 120,000 patients. Am J Gastroenterol. 2009;104:1524–1532. - PubMed
-
- Elster K. Histologic classification of gastric polyps. Curr Top Pathol. 1976;63:77–93. - PubMed
-
- el-Zimaity HM, Jackson FW, Graham DY. Fundic gland polyps developing during omeprazole therapy. Am J Gastroenterol. 1997;92:1858–1860. - PubMed
-
- Raghunath AS, O’Morain C, McLoughlin RC. Review article: the long-term use of proton-pump inhibitors. Aliment Pharmacol Ther. 2005;22(Suppl 1):55–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
