

A colorectal cancer classification system that associates cellular phenotype and responses to therapy
- PMID: 23584089
- PMCID: PMC3774607
- DOI: 10.1038/nm.3175
A colorectal cancer classification system that associates cellular phenotype and responses to therapy
Abstract
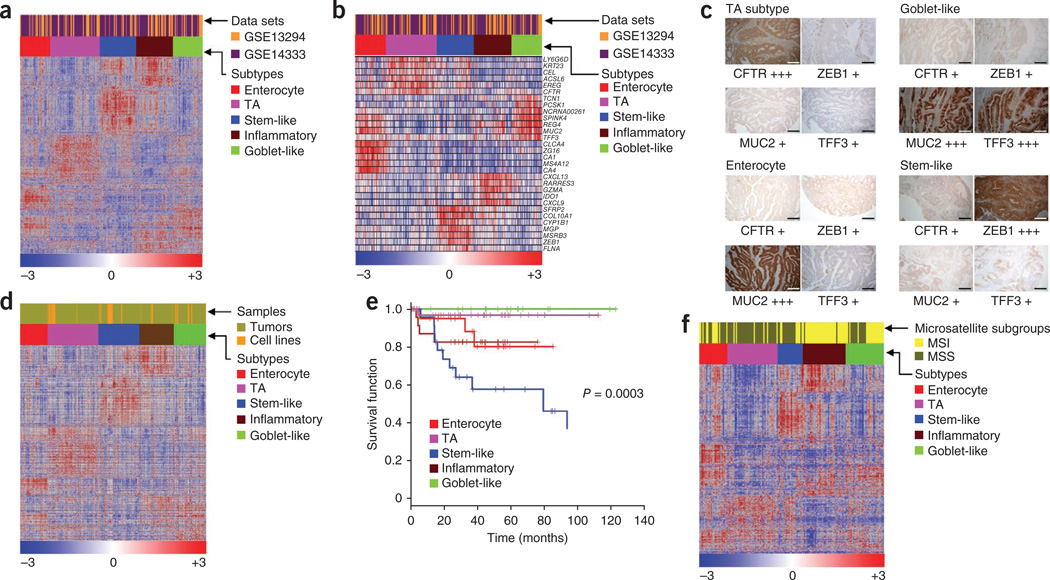
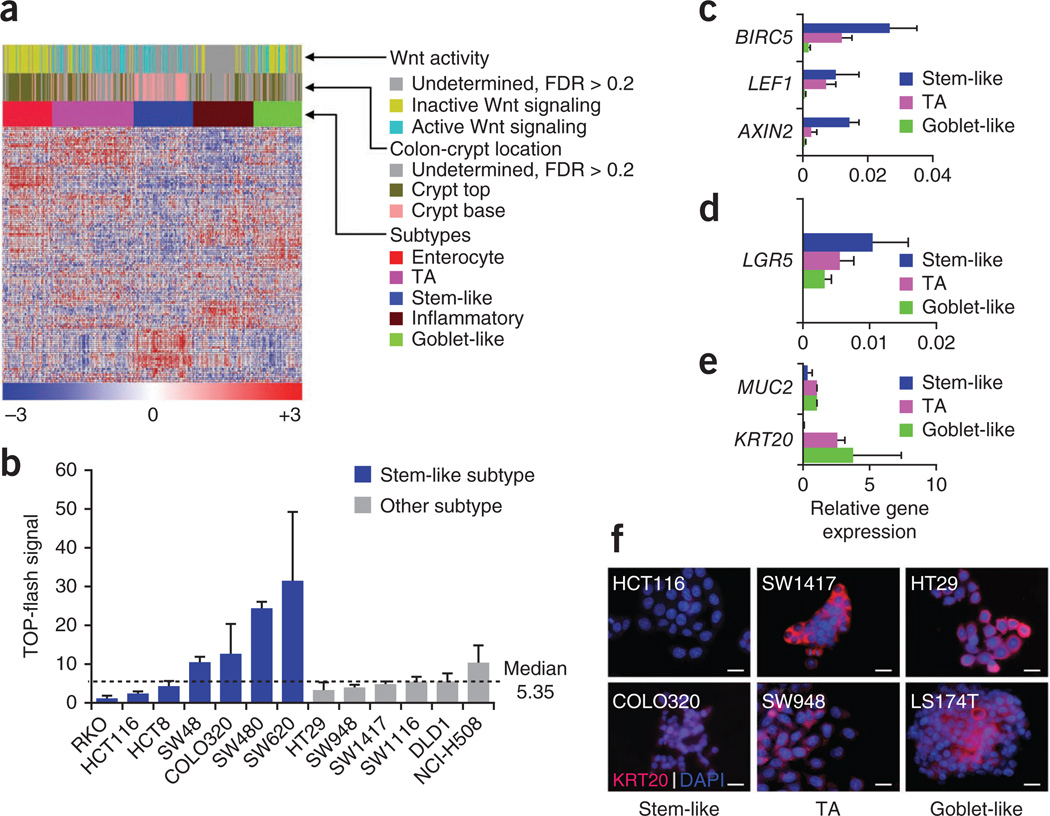
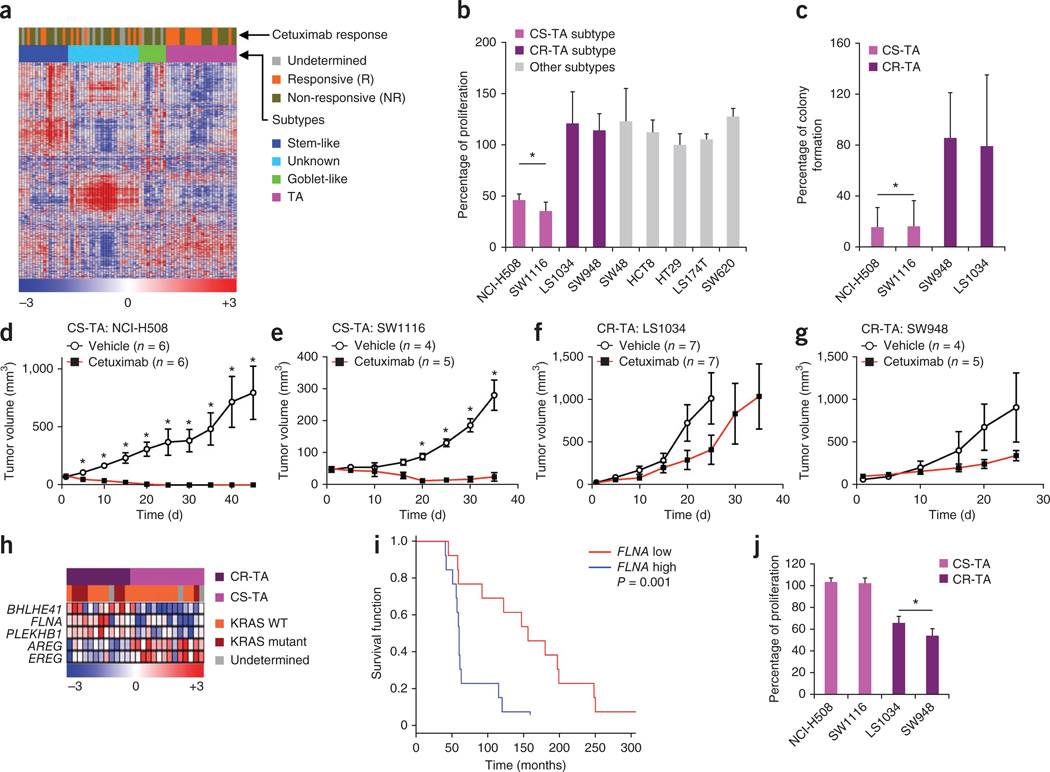
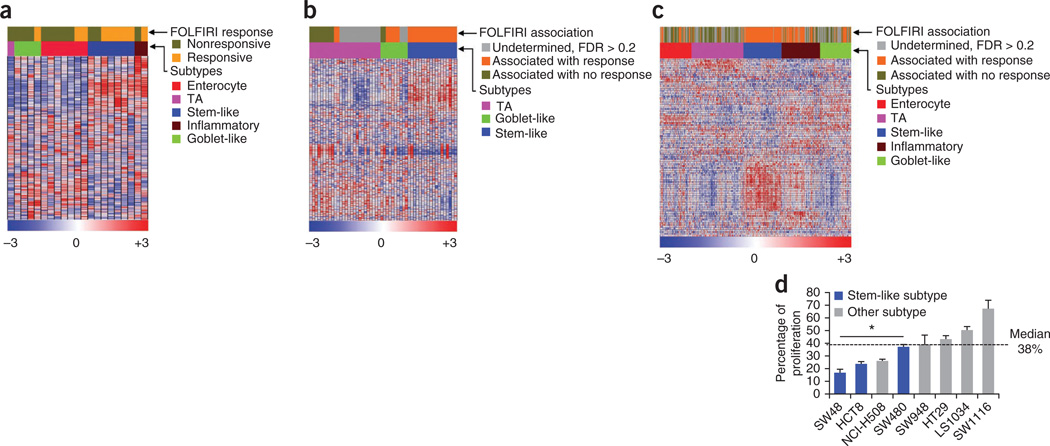
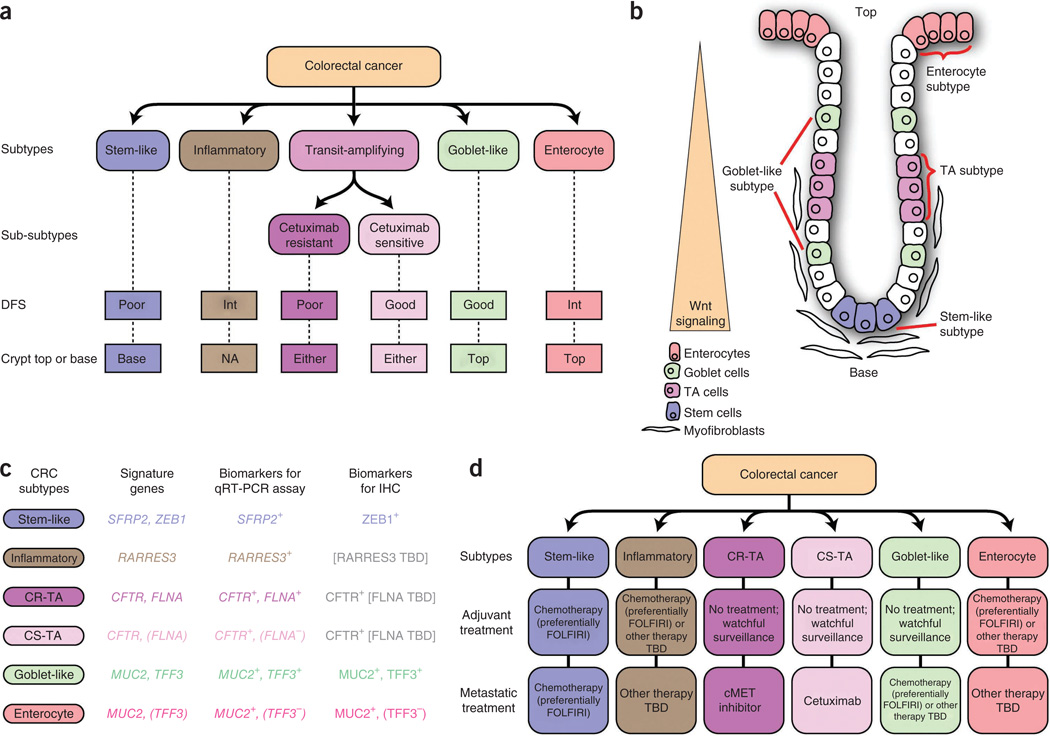
Colorectal cancer (CRC) is a major cause of cancer mortality. Whereas some patients respond well to therapy, others do not, and thus more precise, individualized treatment strategies are needed. To that end, we analyzed gene expression profiles from 1,290 CRC tumors using consensus-based unsupervised clustering. The resultant clusters were then associated with therapeutic response data to the epidermal growth factor receptor-targeted drug cetuximab in 80 patients. The results of these studies define six clinically relevant CRC subtypes. Each subtype shares similarities to distinct cell types within the normal colon crypt and shows differing degrees of 'stemness' and Wnt signaling. Subtype-specific gene signatures are proposed to identify these subtypes. Three subtypes have markedly better disease-free survival (DFS) after surgical resection, suggesting these patients might be spared from the adverse effects of chemotherapy when they have localized disease. One of these three subtypes, identified by filamin A expression, does not respond to cetuximab but may respond to cMET receptor tyrosine kinase inhibitors in the metastatic setting. Two other subtypes, with poor and intermediate DFS, associate with improved response to the chemotherapy regimen FOLFIRI in adjuvant or metastatic settings. Development of clinically deployable assays for these subtypes and of subtype-specific therapies may contribute to more effective management of this challenging disease.
Figures
Comment in
-
Gene expression: colorectal cancer classifications.Nat Rev Cancer. 2013 Jun;13(6):380-1. doi: 10.1038/nrc3529. Epub 2013 May 3. Nat Rev Cancer. 2013. PMID: 23640209 No abstract available.
-
Gastrointestinal cancer: turning up trumps for new CRC subtypes.Nat Rev Clin Oncol. 2013 Jun;10(6):303. doi: 10.1038/nrclinonc.2013.71. Epub 2013 May 7. Nat Rev Clin Oncol. 2013. PMID: 23648824 No abstract available.
-
Colorectal cancer: Is the new era of colorectal cancer classification finally here?Nat Rev Gastroenterol Hepatol. 2013 Jul;10(7):391-3. doi: 10.1038/nrgastro.2013.90. Epub 2013 May 21. Nat Rev Gastroenterol Hepatol. 2013. PMID: 23689082 No abstract available.
-
Reconciliation of classification systems defining molecular subtypes of colorectal cancer: interrelationships and clinical implications.Cell Cycle. 2014;13(3):353-7. doi: 10.4161/cc.27769. Epub 2014 Jan 9. Cell Cycle. 2014. PMID: 24406433 Free PMC article.
-
Colorectal cancer classification based on gene expression is not associated with FOLFIRI response.Nat Med. 2014 Nov;20(11):1230-1. doi: 10.1038/nm.3701. Nat Med. 2014. PMID: 25375918 No abstract available.
-
Reply to Colorectal cancer classification based on gene expression is not associated with FOLFIRI response.Nat Med. 2014 Nov;20(11):1231-2. doi: 10.1038/nm.3742. Nat Med. 2014. PMID: 25375919 No abstract available.
References
-
- Andre T, et al. CPT-11 (irinotecan) addition to bimonthly, high-dose leucovorin and bolus and continuous-infusion 5-fuorouracil (FOLFIRI) for pretreated metastatic colorectal cancer. GERCOR. Eur. J. Cancer. 1999;35:1343–1347. - PubMed
-
- Perou CM, et al. Molecular portraits of human breast tumours. Nature. 2000;406:747–752. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
