

Diagnostic management of patients with suspected ocular sarcoidosis
- PMID: 23585938
- PMCID: PMC3621943
- DOI: 10.3978/j.issn.2072-1439.2013.02.06
Diagnostic management of patients with suspected ocular sarcoidosis
Abstract
Background: Ophthalmologists often refer patients with suspected ocular sarcoidosis to pulmonologists for diagnostic examination of sarcoidosis. However, no recommendation has been proposed for managing such patients. This study aims to prospectively evaluate the diagnostic values of examinations and propose the management of patients with suspected ocular sarcoidosis.
Methods: Consecutive patients with suspected ocular sarcoidosis were prospectively investigated according to type of ocular lesions, measurement of serum ACE, and findings of chest radiography, chest CT, bronchoalveolar lavage (BAL) and transbronchial lung biopsy (TBLB). Diagnostic values were calculated on the basis of pathological results.
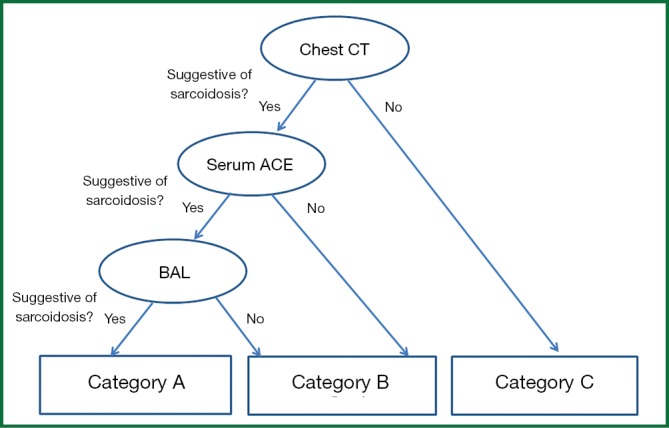
Results: Forty-two patients were included (female, 71.4%; mean age, 56.2±14.8 years), of whom 64.3% was diagnosed with sarcoidosis. Patient characteristics and ocular lesions did not differ significantly, regardless of the presence of sarcoidosis. Chest CT had low specificity and very high sensitivity for detecting sarcoidosis; in contrast, chest radiography and direct findings of bronchofiberscopy had high specificity and low sensitivity. Serum ACE and BAL did not have high diagnostic value. A flow chart was proposed to diagnose sarcoidosis, and this chart reduced the requirement of TBLB to 50% in our population. During the median follow-up of 51 months, 7 patients in the sarcoidosis group (25.9%) developed new lesions.
Conclusions: Application of our flow chart appears to detect avoidable TBLB. Development of a more comprehensive flow chart including survey of ocular findings is warranted.
Keywords: Sarcoidosis; diagnosis; examination; ocular sarcoidosis.
Figures
References
-
- Herbort CP, Rao NA, Mochizuki M, et al. International criteria for the diagnosis of ocular sarcoidosis: results of the first International Workshop On Ocular Sarcoidosis (IWOS). Ocul Immunol Inflamm 2009;17:160-9 - PubMed
-
- Costabel U, Hunninghake GW. ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis Statement Committee. American Thoracic Society. European Respiratory Society. World Association for Sarcoidosis and Other Granulomatous Disorders. Eur Respir J 1999;14:735-7 - PubMed
-
- Rizzato G, Angi M, Fraioli P, et al. Uveitis as a presenting feature of chronic sarcoidosis. Eur Respir J 1996;9:1201-5 - PubMed
-
- Foster S. Ocular manifestations of sarcoidosis preceding systemic manifestations. In: Grassi C, Rizzato G, Pozzi E. eds. Sarcoidosis and other granulomatous disorders. Amsterdam: Elsevier, 1988:177-81.
-
- Rothova A, Alberts C, Glasius E, et al. Risk factors for ocular sarcoidosis. Doc Ophthalmol 1989;72:287-96 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous