

Thromboembolic event rate in paroxysmal and persistent atrial fibrillation: data from the GISSI-AF trial
- PMID: 23586654
- PMCID: PMC3639147
- DOI: 10.1186/1471-2261-13-28
Thromboembolic event rate in paroxysmal and persistent atrial fibrillation: data from the GISSI-AF trial
Abstract
Background: Few data on the thromboembolic (TE) risk of paroxysmal and persistent atrial fibrillation (AF) are available. This study aimed to assess the incidence of TE events in paroxysmal and persistent AF.
Methods: We performed a subset post hoc analysis of 771 patients with paroxysmal and 463 with persistent AF enrolled in the multicenter, prospective, randomized, double-blind, placebo-controlled GISSI-AF trial - comparing the efficacy of valsartan versus placebo in preventing AF recurrences - where the choice of antithrombotic treatment was left to the judgment of the referring physician. TE and major outcome events were centrally validated. AF recurrences were detected by frequent clinic visits and a transtelephonic monitoring device with weekly and symptomatic transmissions.
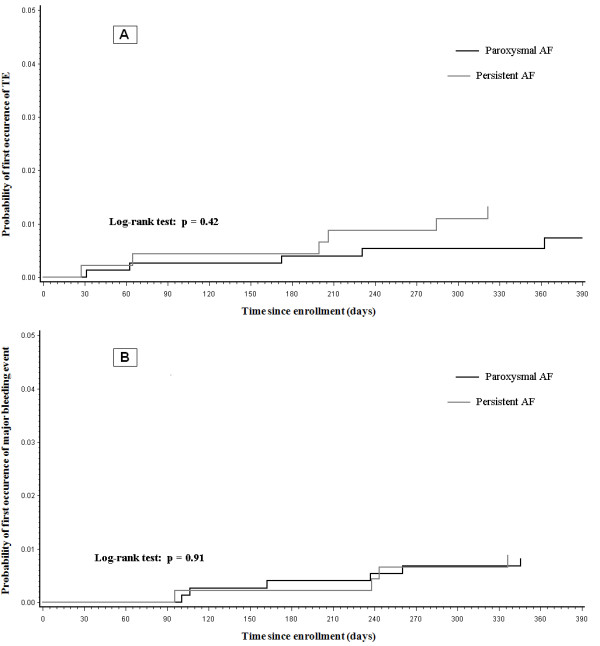
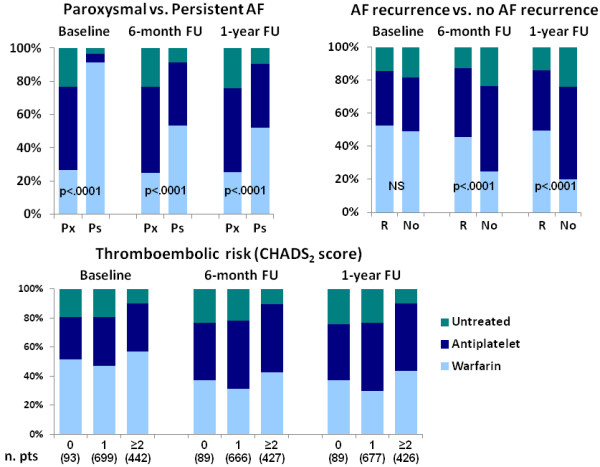
Results: Eighty-five percent of patients had a history of hypertension, and the 7.7% had heart failure, left ventricular dysfunction, or both. The mean CHADS2 score was 1.41±0.84. TE and major bleeding events were observed at a low incidence among the overall population at 1-year follow-up (0.97% and 0.81%, respectively). The univariate and multivariable analyses revealed no statistically significant differences in the incidence of TE, major bleeding events or mortality in paroxysmal and persistent AF patients. TE events were more common among women than men (p=0.02). The follow-up examination showed under- or overtreatment with warfarin in many patients, according to guideline suggestions. Warfarin was more frequently prescribed to patients with persistent AF (p<0.0001) and patients with AF recurrences (p<0.0001). AF recurrences were noninvasively detected in 632 (51.2%) patients. In patients without AF recurrences, the TE event rate was 0.5% versus 1.74%, 1.28%, and 1.18% for those with only symptomatic, only asymptomatic or both symptomatic and asymptomatic AF recurrences, respectively, but the difference was not statistically significant, even after adjusting for warfarin treatment and the CHADS2 score (HR 2.93; CI 95%; 0.8-10.9; p=0.11).
Conclusions: TE and major bleeding events showed a very low incidence in the GISSI-AF trial population, despite under- or overtreatment with warfarin in many patients. TE events had a similar rate in paroxysmal and persistent AF.
Trial registration number: NCT00376272.
Figures
References
-
- Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the European Society of Cardiology committee for practice guidelines: developed in collaboration with the European Heart Rhythm association and the Heart Rhythm Society. Circulation. 2006;114:e257–e354. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
