

Review
doi: 10.1111/apa.12266.
Epub 2013 May 13.
Early recognition of growth abnormalities permitting early intervention
Collaborators,
Affiliations
- PMID: 23586744
- PMCID: PMC3738943
- DOI: 10.1111/apa.12266
Item in Clipboard
Review
Early recognition of growth abnormalities permitting early intervention
Acta Paediatr.
2013 Aug.
Free PMC article
Abstract
Normal growth is a sign of good health. Monitoring for growth disturbances is fundamental to children's health care. Early detection and diagnosis of the causes of short stature allows management of underlying medical conditions, optimizing attainment of good health and normal adult height.
Conclusion: This review summarizes currently available information on monitoring for short stature in children and conditions usually associated with short stature and summarizes the authors' conclusions on the early recognition of growth disorders.
©2013 The Authors. Acta Paediatrica published by John Wiley & Sons Ltd on behalf of Foundation Acta Paediatrica.
Figures
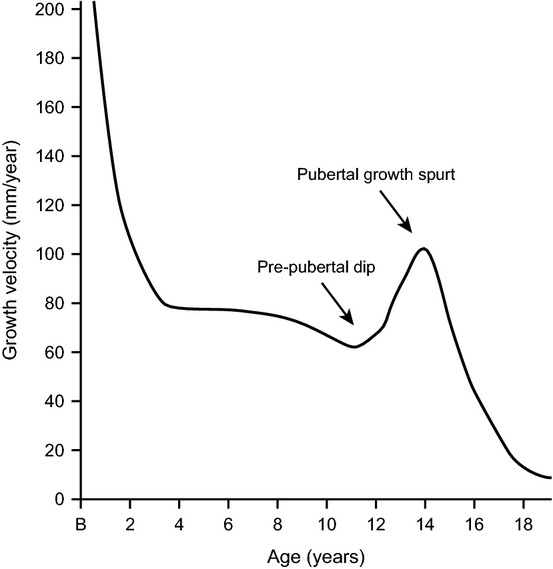
A typical growth velocity curve. Growth is fast in early childhood and then slows down until the start of the pubertal growth spurt.
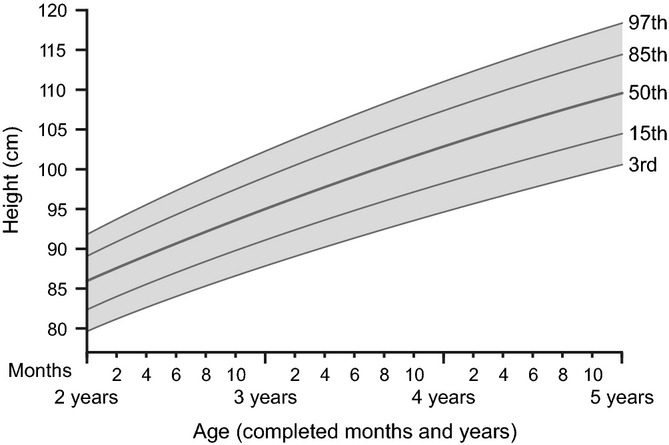
Length-for-age percentiles for girls, from 2 to 5 years. The 50th percentile line (the population average) shows that 50% of normal girls have height (or stature) shorter than the line and 50% are taller. At the lowest line (5th percentile), only 5% of the population of girls/boys are shorter. The growth curves were constructed using data from the WHO Child Growth Study, World Health Organization, Geneva, 2006.
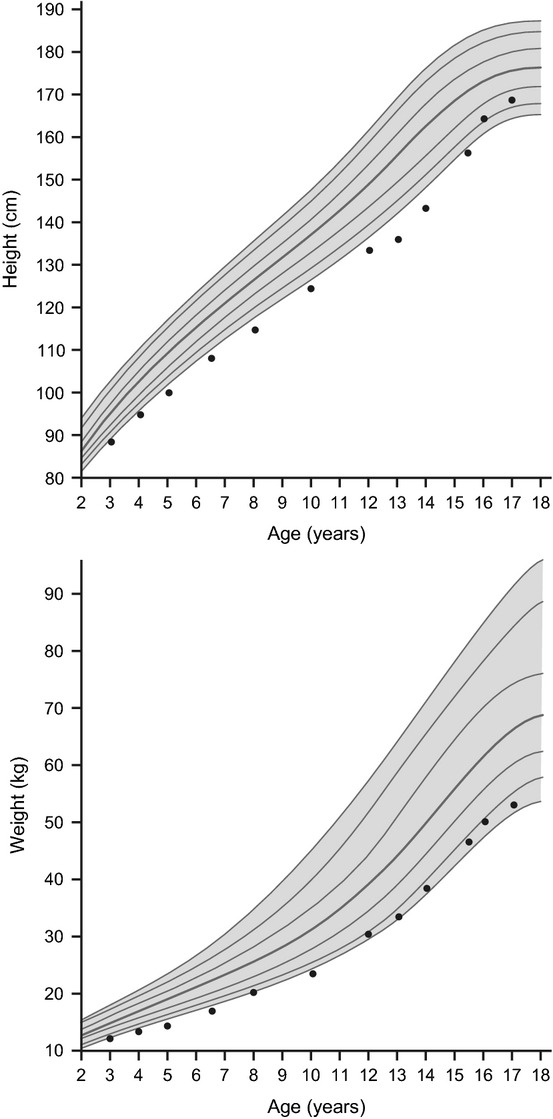
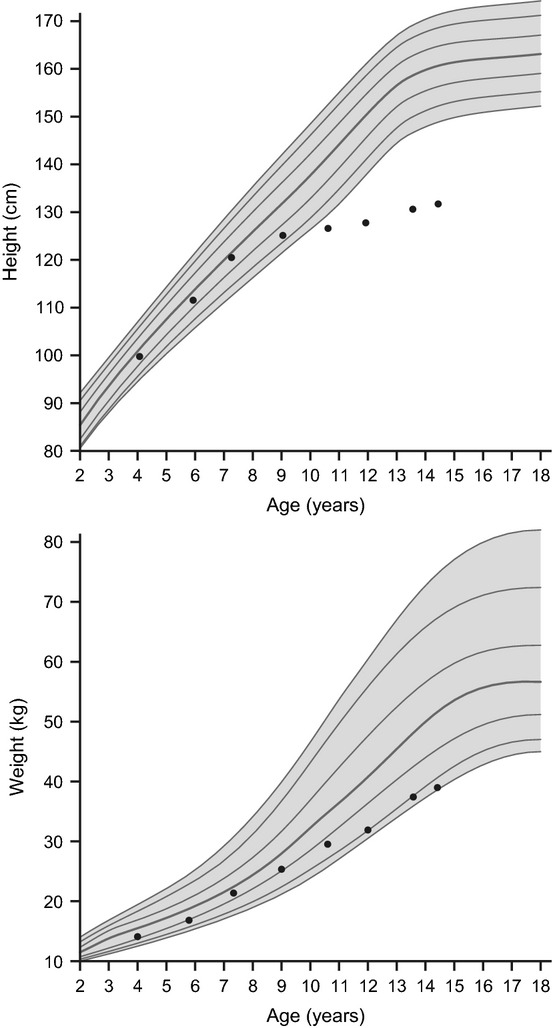
Constitutional growth delay (CGD). Children with CGD, the most common cause of short stature and pubertal delay, typically have retarded linear growth within the first 3 years of life. In this variant of normal growth, linear growth velocity and weight gain slows, beginning as young as 3–6 months, resulting in downward crossing of growth percentiles which often continues until 2–3 years of age. At that time, growth resumes at a normal rate, and these children grow either along the lower growth percentiles or beneath the curve but parallel to it for the remainder of the prepubertal years. At the expected time of puberty, the height of children with CGD begins to drift further from the growth curve because of delay in the onset of the pubertal growth spurt. Catch-up growth, onset of puberty and pubertal growth spurt occur later than average, resulting in normal adult stature and sexual development. Data are for a representative growth curve showing the 3rd, 10th, 25th, 50th, 75th, 90th, 97th percentiles. Dots show a typical growth curve for a child with CGD.
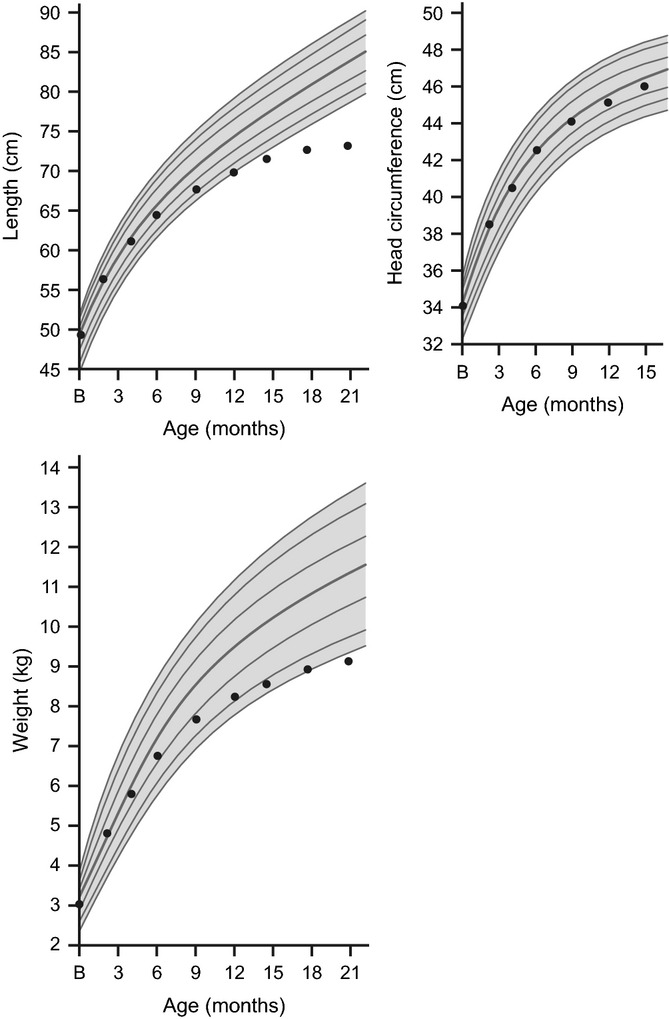
Severe growth hormone deficiency (GHD). If weight and height growth are delayed with a normal head circumference, an endocrinopathy, such as GHD, is suspected. Children with GHD have a slow or flat rate of growth, usually < 2 inches (5 cm) per year. The slow growth may not appear until a child is 2–3 years old. The child will be much shorter than most or all children of the same age and gender. Data are for a representative growth curve showing the 3rd, 10th, 25th, 50th, 75th, 90th, 97th percentiles. Dots show a typical growth curve for a child with GHD.
Acquired hypothyroidism. Short stature and decreasing percentiles dating from the onset of hypothyroidism are characteristic of the condition. Data are for a representative growth curve showing the 3rd, 10th, 25th, 50th, 75th, 90th, 97th percentiles. Dots show a typical growth curve for a child with hypothyroidism.
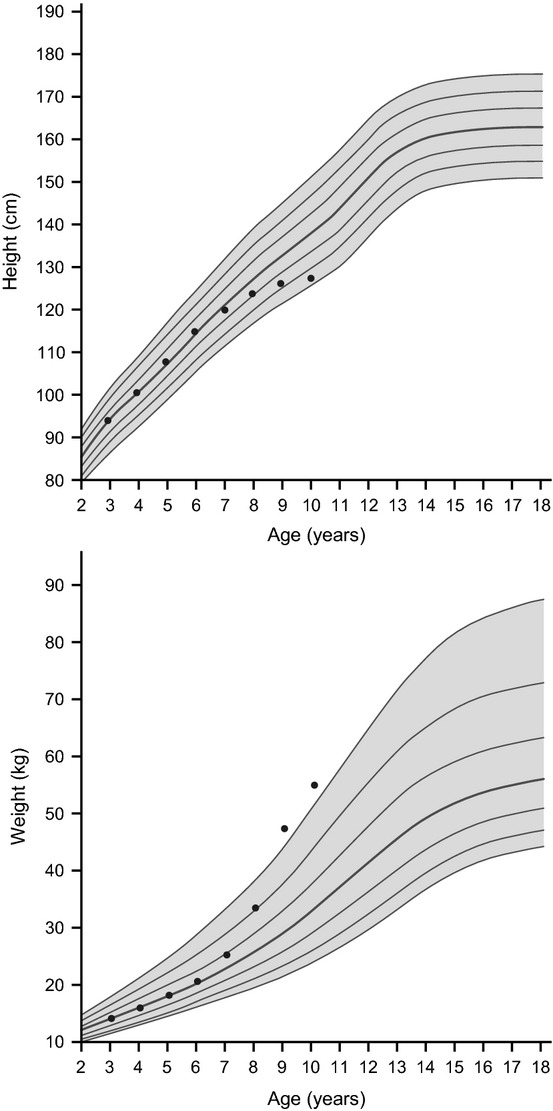
Children with Cushing syndrome characteristically demonstrate an increase in weight velocity with a concomitant decrease in height velocity. Data are for a representative growth curve showing the 3rd, 10th, 25th, 50th, 75th, 90th, 97th percentiles. Dots show a typical growth curve for a child with Cushing syndrome.
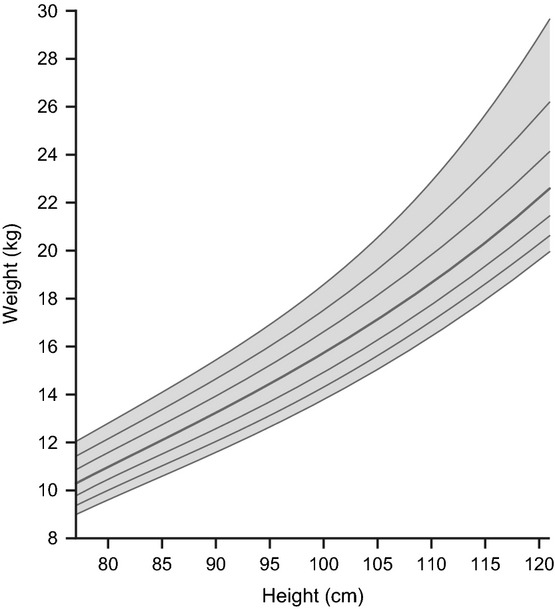
Individual growth chart 3rd, 10th, 25th, 50th, 75th, 90th, 97th percentiles: Boys weight-for-stature. Reproduced from Kuczmarski RJ, Ogden CL, Guo SS et al. 2000 CDC growth charts for the United States: Methods and development. National Center for Health Statistics. Vital Health Stat 2002; 11(246).
References
-
- Thomas M, Massa G, Craen M, de Zegher F, Bourguignon JP, Heinrichs C, et al. Prevalence and demographic features of childhood growth hormone deficiency in Belgium during the period 1986–2001. Eur J Endocrinol. 2004;151:67–72. - PubMed
-
- Sultan M, Afzal M, Qureshi SM, Aziz S, Lutfullah M, Khan SA, et al. Etiology of short stature in children. J Coll Physicians Surg Pak. 2008;18:493–7. - PubMed
-
- Papadimitriou A, Douros K, Papadimitriou DT, Kleanthous K, Karapanou O, Fretzayas A. Characteristics of the short children referred to an academic paediatric endocrine clinic in Greece. J Paediatr Child Health. 2012;48:263–7. - PubMed
-
- Wit JM, Clayton PE, Rogol AD, Savage MO, Saenger PH, Cohen P. Idiopathic short stature: definition, epidemiology, and diagnostic evaluation. Growth Horm IGF Res. 2008;18:89–110. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
