

Thrombelastography (TEG®): practical considerations on its clinical use in trauma resuscitation
- PMID: 23587157
- PMCID: PMC3637505
- DOI: 10.1186/1757-7241-21-29
Thrombelastography (TEG®): practical considerations on its clinical use in trauma resuscitation
Abstract
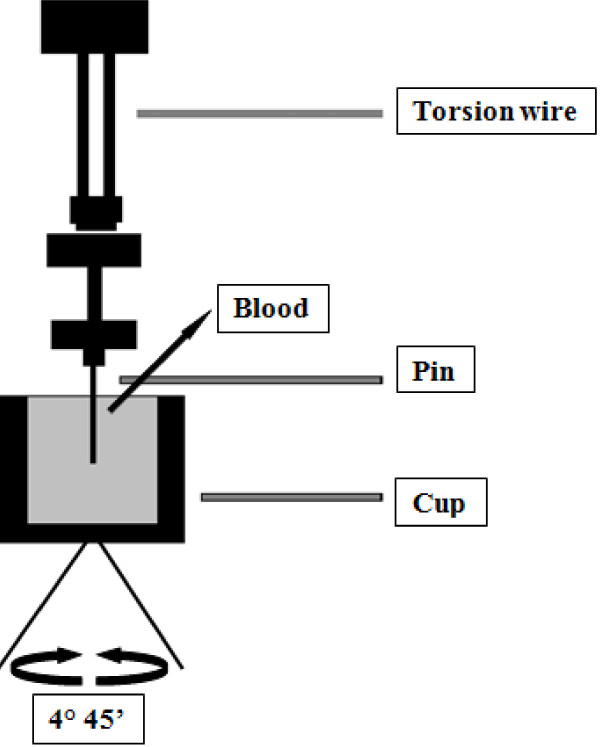
Background: Thrombelastography is a laboratorial test that measures viscoelastic changes of the entire clotting process. There is growing interest in its clinical use in trauma resuscitation, particularly for managing acute coagulopathy of trauma and assisting decision making concerning transfusion. This review focuses on the clinical use of thrombelastography in trauma, with practical points to consider on its use in civilian and military settings.
Methods: A search in the literature using the terms "thrombelastography AND trauma" was performed in PUBMED database. We focused the review on the main clinical aspects of this viscoelastic method in diagnosing and treating patients with acute coagulopathy of trauma during initial resuscitation.
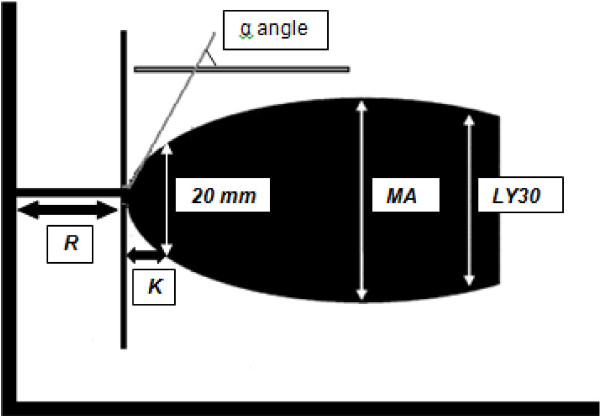
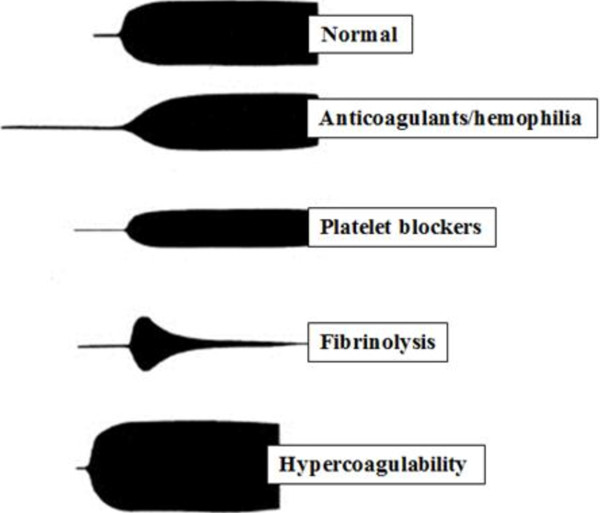
Results: Thrombelastography is not a substitute for conventional laboratorial tests such as INR and aPTT but offers additional information and may guide blood transfusion. Thrombelastography can be used as a point of care test but requires multiple daily calibrations, should be performed by trained personnel and its technique requires standardization. While useful partial results may be available in minutes, the whole test may take as long as other conventional tests. The most important data provided by thrombelastography are clot strength and fibrinolysis. Clot strength measure can establish whether the bleeding is due to coagulopathy or not, and is the key information in thrombelastography-based transfusion algorithms. Thrombelastography is among the few tests that diagnose and quantify fibrinolysis and thus guide the use of anti-fibrinolytic drugs and blood products such as cryoprecipitate and fibrinogen concentrate. It may also diagnose platelet dysfunction and hypercoagulability and potentially prevent inappropriate transfusions of hemostatic blood products to non-coagulopathic patients.
Conclusions: Thrombelastography has characteristics of an ideal coagulation test for use in early trauma resuscitation. It has limitations, but may prove useful as an additional test. Future studies should evaluate its potential to guide blood transfusion and the understanding of the mechanisms of trauma coagulopathy.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
