

HLA-A 31:01 and HLA-B 15:02 as genetic markers for carbamazepine hypersensitivity in children
- PMID: 23588310
- PMCID: PMC3839910
- DOI: 10.1038/clpt.2013.55
HLA-A 31:01 and HLA-B 15:02 as genetic markers for carbamazepine hypersensitivity in children
Abstract
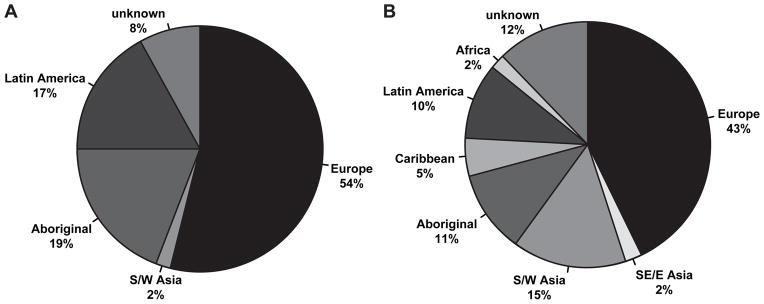
The occurrence of hypersensitivity reactions including rare but life-threatening Stevens-Johnson syndrome (SJS) and drug-induced hypersensitivity syndrome (HSS) limits the use of the anticonvulsant carbamazepine (CBZ). Human leukocyte antigen-B (HLA)-B 15:02 and HLA-A 31:01 have been identified as predictive genetic markers for CBZ hypersensitivity in Asian and European patients. To replicate these genetic associations in pediatric patients from North America with a diverse ethnic background, we investigated HLA-A 31:01 and HLA-B 15:02 in 42 children with CBZ hypersensitivity and 91 CBZ-tolerant children from across Canada. HLA-A 31:01 was significantly associated with CBZ-HSS (odds ratio (OR): 26.4, P = 0.0025) and maculopapular exanthema (MPE) (OR: 8.6, P = 0.0037) but not with CBZ-SJS. Conversely, HLA-B 15:02 was associated with CBZ-SJS (OR: 38.6, P = 0.002) but not HSS or MPE. This study is the first to demonstrate the association of HLA-A 31:01 with CBZ hypersensitivity in children, providing important replication of this association and highlighting the importance of HLA-A 31:01 as a predictive biomarker across various ancestries.
Conflict of interest statement
MJR holds the CIHR-GSK Chair in Pediatric Clinical Pharmacology at the University of Western Ontario; NHS has been a paid consultant for Novartis; the other authors declared no financial relationships or conflicts of interest relevant to this article.
Figures
References
-
- Landmark CJ, Fossmark H, Larsson PG, Rytter E, Johannessen SI. Prescription patterns of antiepileptic drugs in patients with epilepsy in a nation-wide population. Epilepsy Res. 2011;95:51–9. - PubMed
-
- van de Vrie-Hoekstra NW, de Vries TW, van den Berg PB, Brouwer OF, de Jong-van den Berg LT. Antiepileptic drug utilization in children from 1997–2005--a study from the Netherlands. Eur J Clin Pharmacol. 2008;64:1013–20. - PubMed
-
- Wheless JW, Clarke DF, Arzimanoglou A, Carpenter D. Treatment of pediatric epilepsy: European expert opinion, 2007. Epileptic Disord. 2007;9:353–412. - PubMed
-
- Wheless JW, Clarke DF, Carpenter D. Treatment of pediatric epilepsy: expert opinion, 2005. J Child Neurol. 2005;20(Suppl 1):S1–56. quiz S9–60. - PubMed
-
- Segal AR, Doherty KM, Leggott J, Zlotoff B. Cutaneous reactions to drugs in children. Pediatrics. 2007;120:e1082–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
