

Portfolios of biomedical HIV interventions in South Africa: a cost-effectiveness analysis
- PMID: 23588668
- PMCID: PMC3785647
- DOI: 10.1007/s11606-013-2417-1
Portfolios of biomedical HIV interventions in South Africa: a cost-effectiveness analysis
Abstract
Background: Recent clinical trials of male circumcision, oral pre-exposure prophylaxis (PrEP), and a vaginal microbicide gel have shown partial effectiveness at reducing HIV transmission, stimulating interest in implementing portfolios of biomedical prevention programs.
Objective: To evaluate the effectiveness and cost-effectiveness of combination biomedical HIV prevention and treatment scale-up in South Africa, given uncertainty in program effectiveness.
Design: Dynamic HIV transmission and disease progression model with Monte Carlo simulation and cost-effectiveness analysis.
Participants: Men and women aged 15 to 49 years in South Africa.
Interventions: HIV screening and counseling, antiretroviral therapy (ART), male circumcision, PrEP, microbicide, and select combinations.
Main measures: HIV incidence, prevalence, discounted costs, discounted quality-adjusted life years (QALYs), and incremental cost-effectiveness ratios.
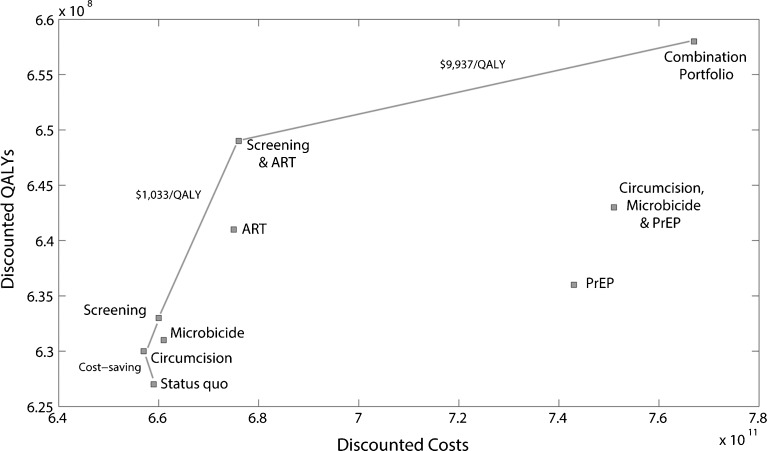
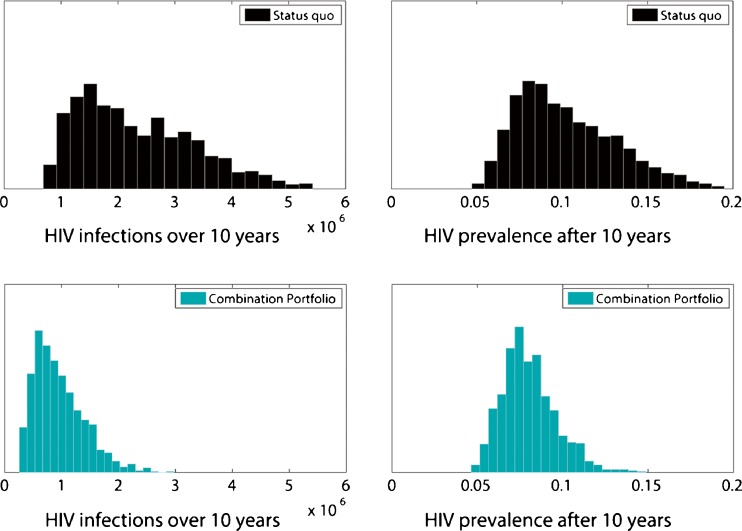
Key results: Providing half of all uninfected persons with PrEP averts 28 % of future HIV infections for $9,000/QALY gained, but the affordability of such a program is questionable. Given limited resources, annual HIV screening and ART utilization by 75 % of eligible infected persons could avert one-third of new HIV infections, for approximately $1,000/QALY gained. Male circumcision is more cost-effective, but disproportionately benefits men. A comprehensive portfolio of expanded screening, ART, male circumcision, microbicides, and PrEP could avert 62 % of new HIV infections, reducing HIV prevalence from a projected 14 % to 10 % after 10 years. This strategy doubles treatment initiation and adds 31 million QALYs to the population. Despite uncertainty in program effectiveness, a comprehensive portfolio costs less than $10,000/QALY gained in 33 % of simulation iterations and less than $30,000/QALY gained in 90 % of iterations, assuming an annual microbicide cost of $100.
Conclusions: A portfolio of modestly-effective biomedical HIV prevention programs, including male circumcision, vaginal microbicides, and oral PrEP, could substantially reduce HIV incidence and prevalence in South Africa and be likely cost-effective. Given limited resources, PrEP is the least cost-effective intervention of those considered.
Figures


Comment in
-
Capsule commentary on Long and Stavert, portfolios of biomedical HIV interventions in South Africa: a cost-effectiveness analysis.J Gen Intern Med. 2013 Oct;28(10):1350. doi: 10.1007/s11606-013-2519-9. J Gen Intern Med. 2013. PMID: 23860721 Free PMC article. No abstract available.
Similar articles
-
Effectiveness and cost effectiveness of oral pre-exposure prophylaxis in a portfolio of prevention programs for injection drug users in mixed HIV epidemics.PLoS One. 2014 Jan 28;9(1):e86584. doi: 10.1371/journal.pone.0086584. eCollection 2014. PLoS One. 2014. PMID: 24489747 Free PMC article.
-
The cost-effectiveness of preexposure prophylaxis for HIV prevention in the United States in men who have sex with men.Ann Intern Med. 2012 Apr 17;156(8):541-50. doi: 10.7326/0003-4819-156-8-201204170-00001. Ann Intern Med. 2012. PMID: 22508731 Free PMC article.
-
Comparative effectiveness and cost-effectiveness of antiretroviral therapy and pre-exposure prophylaxis for HIV prevention in South Africa.BMC Med. 2014 Mar 17;12:46. doi: 10.1186/1741-7015-12-46. BMC Med. 2014. PMID: 24629217 Free PMC article.
-
Where to deploy pre-exposure prophylaxis (PrEP) in sub-Saharan Africa?Sex Transm Infect. 2013 Dec;89(8):628-34. doi: 10.1136/sextrans-2012-050891. Epub 2013 Aug 2. Sex Transm Infect. 2013. PMID: 23912819 Review.
-
Cost-effectiveness of pre-exposure prophylaxis for HIV: a review.Curr Opin HIV AIDS. 2012 Nov;7(6):587-92. doi: 10.1097/COH.0b013e3283582c8b. Curr Opin HIV AIDS. 2012. PMID: 23076124 Review.
Cited by
-
Prospects for HIV control in South Africa: a model-based analysis.Glob Health Action. 2016 Jun 8;9:30314. doi: 10.3402/gha.v9.30314. eCollection 2016. Glob Health Action. 2016. PMID: 27282146 Free PMC article.
-
Capsule commentary on Long and Stavert, portfolios of biomedical HIV interventions in South Africa: a cost-effectiveness analysis.J Gen Intern Med. 2013 Oct;28(10):1350. doi: 10.1007/s11606-013-2519-9. J Gen Intern Med. 2013. PMID: 23860721 Free PMC article. No abstract available.
-
"This is the medicine:" A Kenyan community responds to a sexual concurrency reduction intervention.Soc Sci Med. 2014 May;108:175-84. doi: 10.1016/j.socscimed.2014.01.039. Epub 2014 Feb 4. Soc Sci Med. 2014. PMID: 24650739 Free PMC article.
-
Implementation and resource needs for long-acting PrEP in low- and middle-income countries: a scoping review.J Int AIDS Soc. 2023 Jul;26 Suppl 2(Suppl 2):e26110. doi: 10.1002/jia2.26110. J Int AIDS Soc. 2023. PMID: 37439063 Free PMC article.
-
Potential Impact and Cost-Effectiveness of Condomless-Sex-Concentrated PrEP in KwaZulu-Natal Accounting for Drug Resistance.J Infect Dis. 2021 Apr 23;223(8):1345-1355. doi: 10.1093/infdis/jiz667. J Infect Dis. 2021. PMID: 31851759 Free PMC article.
References
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS). Report on the global AIDS epidemic. Geneva 2010.
-
- Kates J, Boortz K, Lief E, Avila C, Bobet G. Financing the Response to AIDS in Low- and Middle-Income Countries: International Assistance from the G8, European Commission and Other Donor Governments in 2009, Washington, DC: Kaiser Family Foundation and UNAIDS; 2010.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
