

Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications
- PMID: 23588747
- PMCID: PMC3736840
- DOI: 10.7326/0003-4819-158-8-201304160-00003
Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications
Abstract
Background: Osteoporosis is a prevalent but underdiagnosed condition.
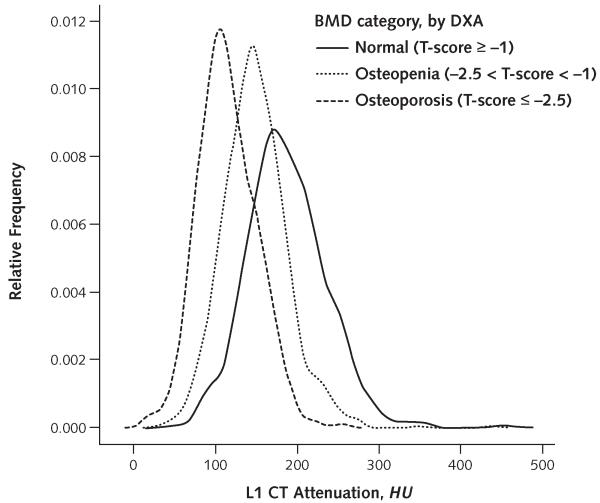
Objective: To evaluate computed tomography (CT)-derived bone mineral density (BMD) assessment compared with dual-energy x-ray absorptiometry (DXA) measures for identifying osteoporosis by using CT scans performed for other clinical indications.
Design: Cross-sectional study.
Setting: Single academic health center.
Patients: 1867 adults undergoing CT and DXA (n = 2067 pairs) within a 6-month period over 10 years.
Measurements: CT-attenuation values (in Hounsfield units [HU]) of trabecular bone between the T12 and L5 vertebral levels, with an emphasis on L1 measures (study test); DXA BMD measures (reference standard). Sagittal CT images assessed for moderate-to-severe vertebral fractures.
Results: CT-attenuation values were significantly lower at all vertebral levels for patients with DXA-defined osteoporosis (P < 0.001). An L1 CT-attenuation threshold of 160 HU or less was 90% sensitive and a threshold of 110 HU was more than 90% specific for distinguishing osteoporosis from osteopenia and normal BMD. Positive predictive values for osteoporosis were 68% or greater at L1 CT-attenuation thresholds less than 100 HU; negative predictive values were 99% at thresholds greater than 200 HU. Among 119 patients with at least 1 moderate-to-severe vertebral fracture, 62 (52.1%) had nonosteoporotic T-scores (DXA false-negative results), and most (97%) had L1 or mean T12 to L5 vertebral attenuation of 145 HU or less. Similar performance was seen at all vertebral levels. Intravenous contrast did not affect CT performance.
Limitation: The potential benefits and costs of using the various CT-attenuation thresholds identified were not formally assessed.
Conclusion: Abdominal CT images obtained for other reasons that include the lumbar spine can be used to identify patients with osteoporosis or normal BMD without additional radiation exposure or cost.
Primary funding source: National Institutes of Health.
Figures







Comment in
-
Conventional computed tomography imaging and bone mineral density: opportunistic screening or "incidentaloporosis"?Ann Intern Med. 2013 Apr 16;158(8):630-1. doi: 10.7326/0003-4819-158-8-201304160-00009. Ann Intern Med. 2013. PMID: 23588751 No abstract available.
References
-
- Raisz LG. Clinical practice. Screening for osteoporosis. N Engl J Med. 2005;353:164–71. [PMID: 16014886] - PubMed
-
- Ebeling PR. Clinical practice. Osteoporosis in men. N Engl J Med. 2008;358:1474–82. [PMID: 18385499] - PubMed
-
- Bessette L, Ste-Marie LG, Jean S, Davison KS, Beaulieu M, Baranci M, et al. The care gap in diagnosis and treatment of women with a fragility fracture. Osteoporos Int. 2008;19:79–86. [PMID: 17641811] - PubMed
-
- King AB, Fiorentino DM. Medicare payment cuts for osteoporosis testing reduced use despite tests’ benefit in reducing fractures. Health Aff (Millwood) 2011;30:2362–70. [PMID: 22147865] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical