

Five-year downstream outcomes following prostate-specific antigen screening in older men
- PMID: 23588999
- PMCID: PMC3712749
- DOI: 10.1001/jamainternmed.2013.323
Five-year downstream outcomes following prostate-specific antigen screening in older men
Abstract
Importance: Despite ongoing controversies surrounding prostate-specific antigen (PSA) screening, many men 65 years or older undergo screening. However, few data exist that quantify the chain of events following screening in clinical practice to better inform decisions.
Objective: To quantify 5-year downstream outcomes following a PSA screening result exceeding 4.0 ng/mL in older men.
Design and setting: Longitudinal cohort study in the national Veterans Affairs health care system.
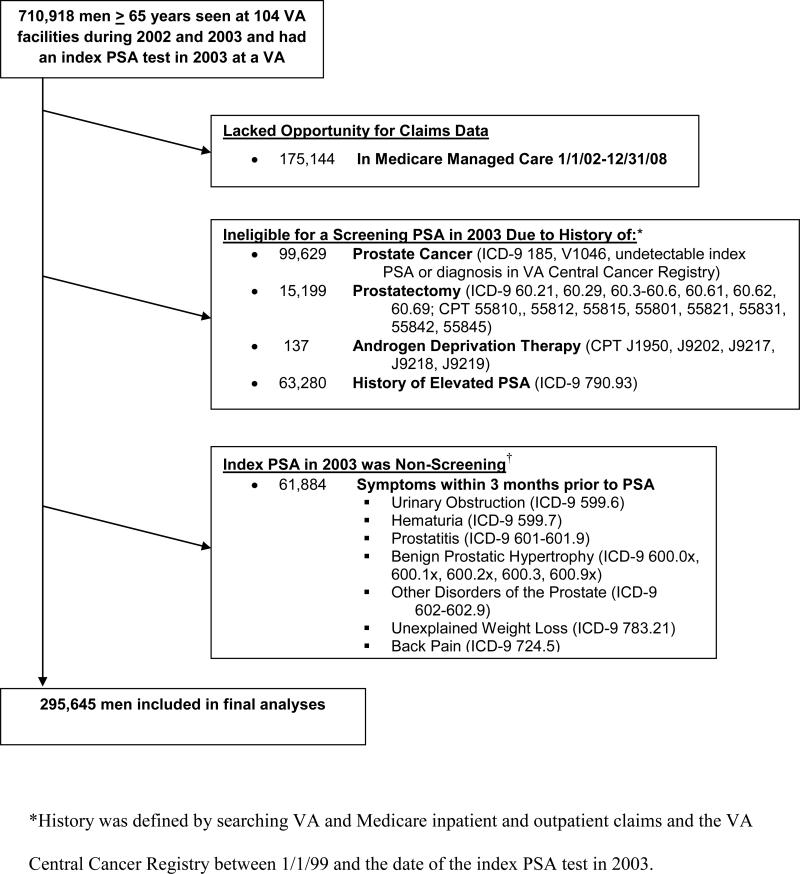
Participants: In total, 295,645 men 65 years or older who underwent PSA screening in the Veterans Affairs health care system in 2003 and were followed up for 5 years using national Veterans Affairs and Medicare data.
Main outcome measures: Among men whose index screening PSA level exceeded 4.0 ng/mL, we determined the number who underwent prostate biopsy, were diagnosed as having prostate cancer, were treated for prostate cancer, and were treated for prostate cancer and were alive at 5 years according to baseline characteristics. Biopsy and treatment complications were also assessed.
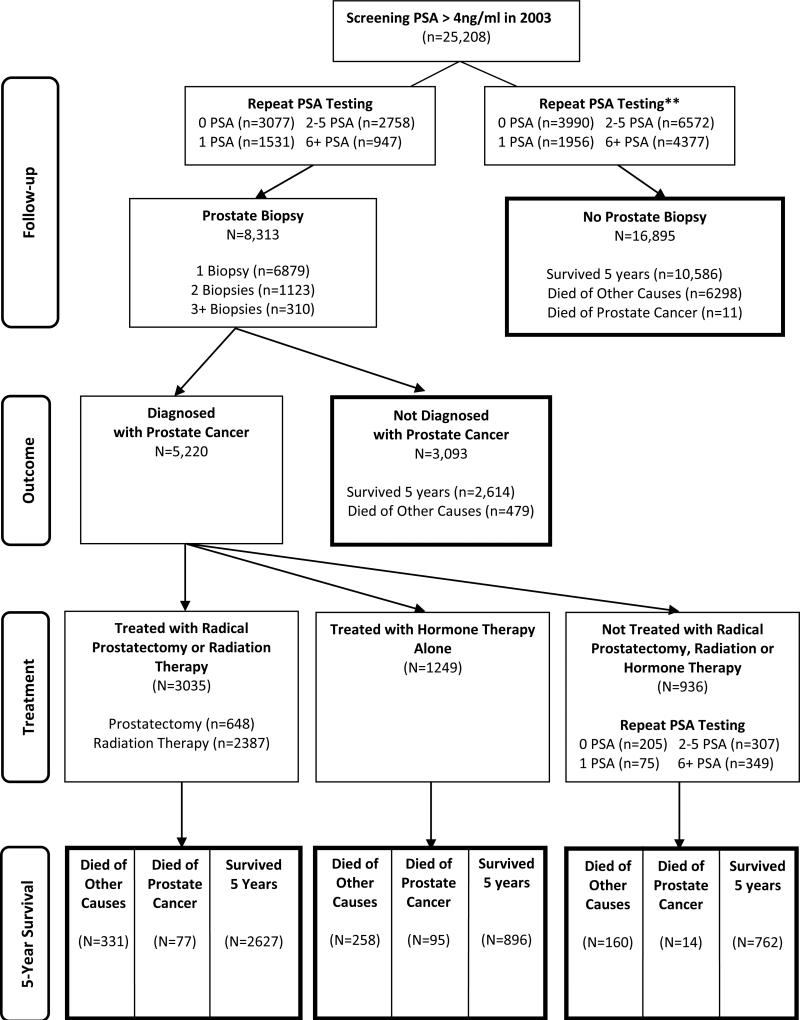
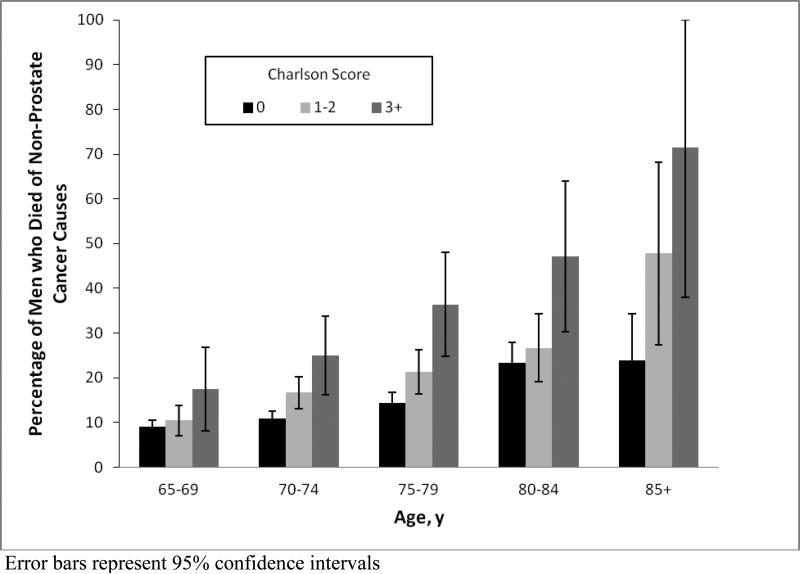
Results: In total, 25,208 men (8.5%) had an index PSA level exceeding 4.0 ng/mL. During the 5-year follow-up period, 8313 men (33.0%) underwent at least 1 prostate biopsy, and 5220 men (62.8%) who underwent prostate biopsy were diagnosed as having prostate cancer, of whom 4284 (82.1%) were treated for prostate cancer. Performance of prostate biopsy decreased with advancing age and worsening comorbidity (P < .001), whereas the percentage treated for biopsy-detected cancer exceeded 75% even among men 85 years or older, those with a Charlson-Deyo Comorbidity Index of 3 or higher, and those having low-risk cancer. Among men with biopsy-detected cancer, the risk of death from non-prostate cancer causes increased with advancing age and worsening comorbidity (P < .001). In total, 468 men (5.6%) had complications within 7 days after prostate biopsy. Complications of prostate cancer treatment included new urinary incontinence in 584 men (13.6%) and new erectile dysfunction 588 men (13.7%).
Conclusions and relevance: Performance of prostate biopsy is uncommon in older men with abnormal screening PSA levels and decreases with advancing age and worsening comorbidity. However, once cancer is detected on biopsy, most men undergo immediate treatment regardless of advancing age, worsening comorbidity, or low-risk cancer. Understanding downstream outcomes in clinical practice should better inform individualized decisions among older men considering PSA screening.
Figures


References
-
- Moyer VA. Screening for prostate cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2012;157 (published on-line) - PubMed
-
- Smith RA, Cokkinides V, Brooks D, Saslow D, Shah M, Brawley OW. Cancer screening in the United States, 2011: a review of current American Cancer Society guidelines and issues in cancer screening. CA Cancer J Clin. 2011;61(1):8–30. - PubMed
-
- Greene KL, Albertsen PC, Babaian RJ, et al. Prostate specific antigen best practice statement: 2009 update. J Urol. 2009;182(5):2232–2241. - PubMed
-
- Walter LC, Bertenthal D, Lindquist K, Konety BR. PSA screening among elderly men with limited life expectancies. JAMA. 2006;296(19):2336–2342. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
