

A dangerous twist of the 'T' wave: A case of Wellens' Syndrome
- PMID: 23589737
- PMCID: PMC3626028
- DOI: 10.4066/AMJ.2013.1636
A dangerous twist of the 'T' wave: A case of Wellens' Syndrome
Abstract
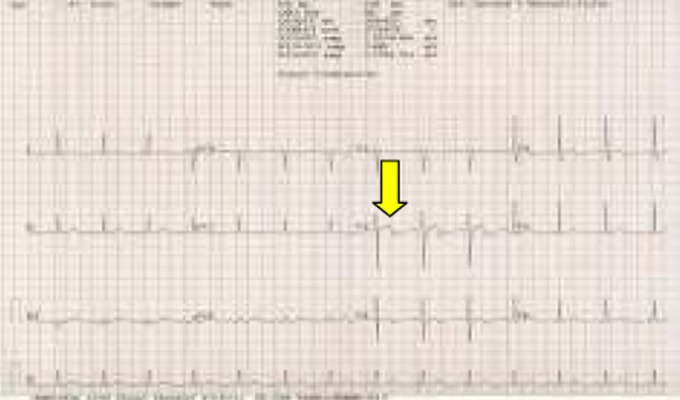
Wellens' syndrome is a condition in which electrocardiographic (ECG) changes indicate critical proximal left anterior descending artery narrowing occurring during the chest pain-free period. Due to the severity of the obstruction, if such cases are managed by early invasive revascularisation therapy, a major threat in the form of a massive myocardial infarction or sudden death may be averted. We present the case of a patient with previous chest pain, whose ECG showing subtle ischemic changes was initially overlooked. A repeat ECG taken during the painless period showed a biphasic T wave, suggestive of Wellen's' syndrome. This was confirmed by an immediate coronary angiogram.
Keywords: Wellens’ syndrome; electrocadiographic changes; left anterior descending artery obstruction; revascularisation.
Figures






References
-
- Kardesoglu E, Celik T, Cebeci BS, Cingozbay BY, Dincturk M, Demiralp E. Wellens' syndrome: a case report. J Int Med Res. 2003 Nov-Dec;31(6):585–90. - PubMed
-
- De Zwaan C, Bär WHM, Wellens HJJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in the left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982 Apr;103(4 Pt 2):730–6. - PubMed
-
- De Zwann C, Bar FW, Janssen JH. et al. Angiographic and clinical characteristics of patients with unstable angina showing an ECG pattern indicating critical narrowing of the proximal LAD coronary artery. Am Heart J. 1982 Apr;103(4 Pt 2):730–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources