

doi: 10.1155/2013/809568.
Epub 2013 Mar 26.
MR Neurography: Advances
Affiliations
- PMID: 23589774
- PMCID: PMC3622412
- DOI: 10.1155/2013/809568
Item in Clipboard
MR Neurography: Advances
Radiol Res Pract.
2013.
Abstract
High resolution and high field magnetic resonance neurography (MR neurography, MRN) is shown to have excellent anatomic capability. There have been considerable advances in the technology in the last few years leading to various feasibility studies using different structural and functional imaging approaches in both clinical and research settings. This paper is intended to be a useful seminar for readers who want to gain knowledge of the advancements in the MRN pulse sequences currently used in clinical practice as well as learn about the other techniques on the horizon aimed at better depiction of nerve anatomy, pathology, and potential noninvasive evaluation of nerve degeneration or regeneration.
Figures
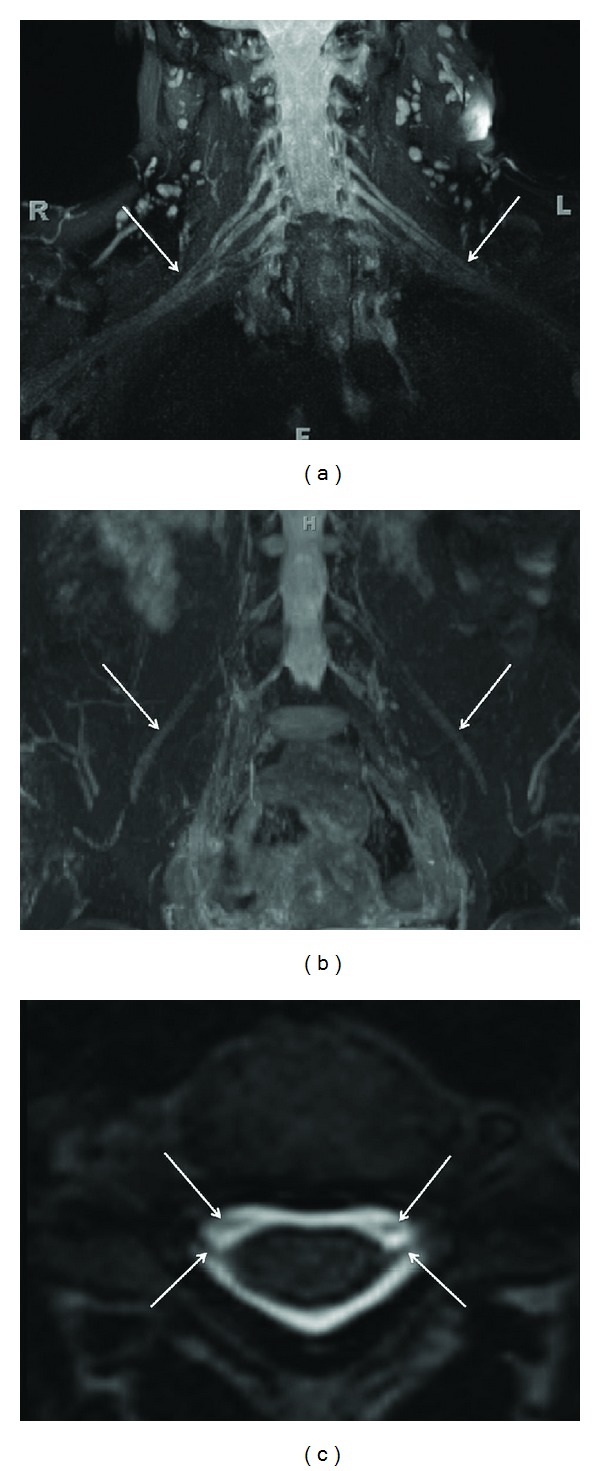
(a) 3D anatomic nonselective MRN-MIP reconstruction from a coronal 3D STIR SPACE sequence shows normal symmetric signal intensity and size of bilateral brachial plexuses (arrows). (b) 3D anatomic nonselective MRN-MIP reconstruction from a coronal 3D STIR SPACE sequence shows normal symmetric signal intensity and size of bilateral LS plexuses and femoral nerves (arrows). (c) 3D anatomic nonselective MRN-Axial reconstruction from 3D T2 SPACE sequence shows the dorsal and ventral roots (preganglionic segments) on both sides (arrows).
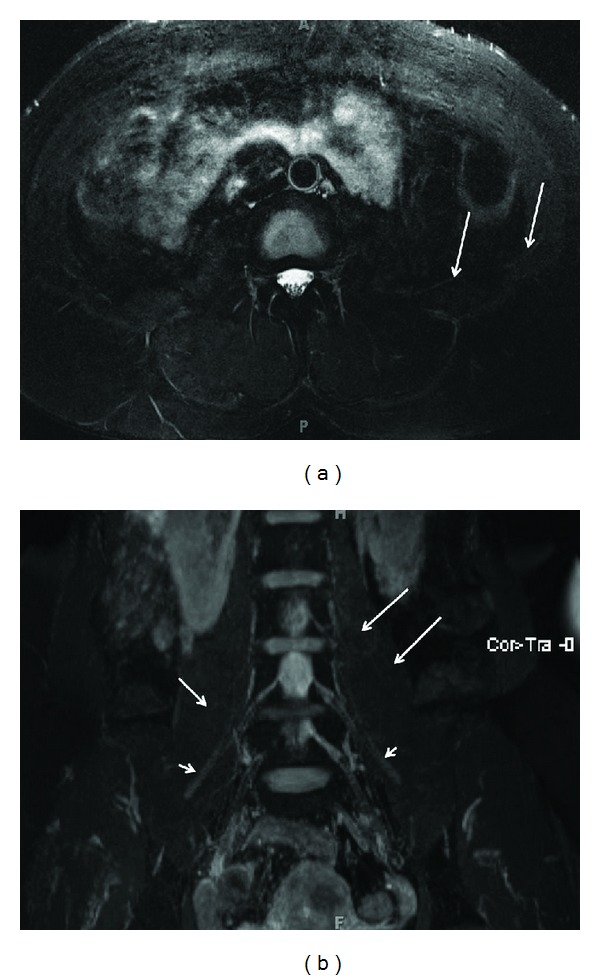
(a) 2D versus 3D anatomic nonselective MRN-Axial T2 SPAIR image through the lower abdomen shows the abnormally hyperintense left ilioinguinal nerve (arrows) in a suspected case of left ilioinguinal neuropathy. (b) 2D versus 3D anatomic nonselective MRN-MIP reconstruction from a coronal 3D STIR SPACE sequence barely shows the left ilioinguinal nerve (large arrows). Notice normal right ilioinguinal nerve (medium arrow) and normal bilateral femoral nerves (small arrows).
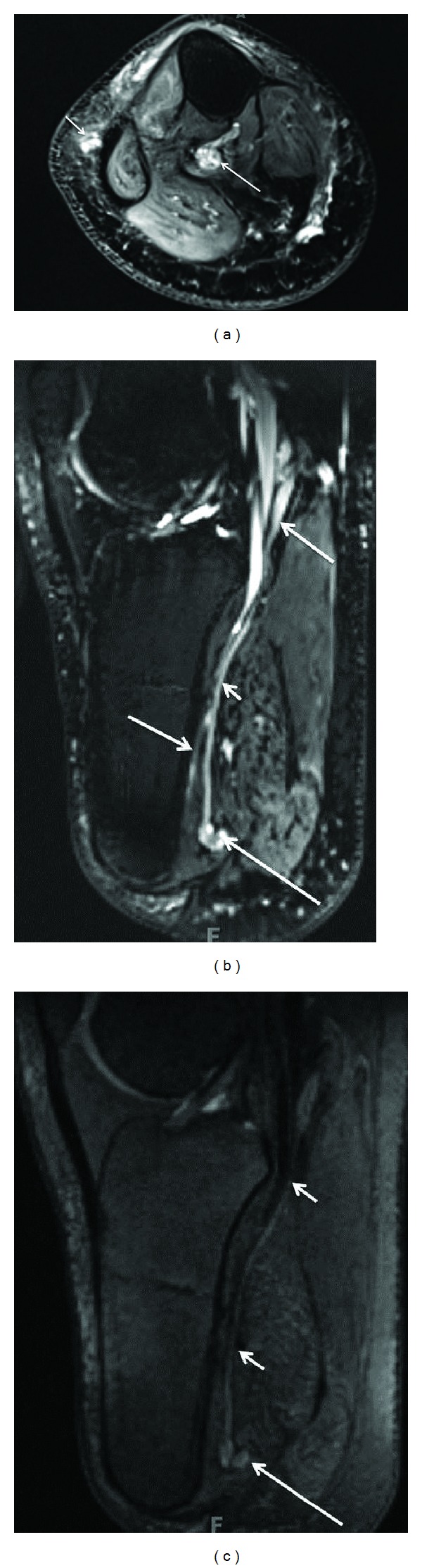
(a) Limitation of 3D anatomic nonselective MRN-Axial T2 SPAIR image through the upper calf shows amputation neuromas of tibial nerve (large arrow) and common peroneal nerve (small arrow). (b) Limitation of 3D anatomic nonselective MRN-Sagittal reconstruction from a 3D SPAIR SPACE sequence in the same case shows the abnormal tibial nerve in its long axis (smaller arrow) with an end-bulb neuroma (large arrow). However, there is suboptimal depiction due to hyperintense vascular signal contamination (medium arrows). (c) 3D anatomic nerve selective MRN-Sagittal reconstruction from a 3D DW PSIF sequence in the same case selectively shows the abnormal tibial nerve in its long axis (small arrows) with an end-bulb neuroma (large arrow).
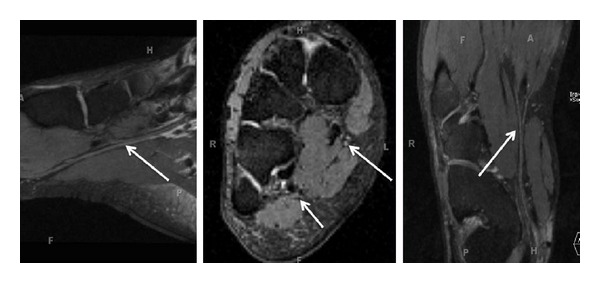
3D anatomic nerve selective MRN-Multiplanar reconstructions from an isotropic 3D DW PSIF sequence through the mid foot shows the normal long axis appearances of the medial plantar nerve (large arrows) and lateral plantar nerve (small arrow).
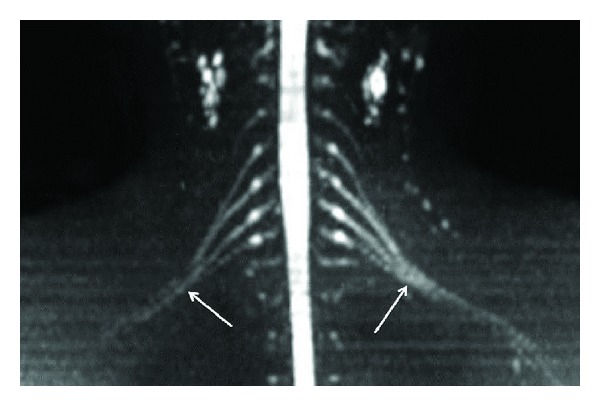
3D anatomic nerve selective MRN-Coronal MIP from a 3D diffusion weighted single shot EPI (b value 800 s/mm2) shows the symmetrical normal appearance of bilateral brachial plexuses (arrows).
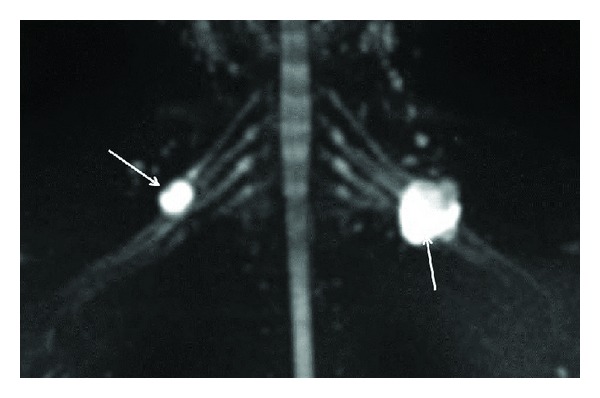
3D anatomic nerve selective MRN-Coronal MIP from a 3D diffusion weighted single shot EPI (b value 800 s/mm2) shows the peripheral nerve sheath tumors originating from the right C5 nerve root and the left upper trunk (arrows).
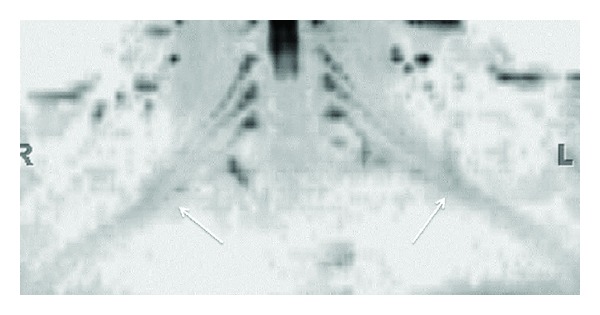
3D functional nerve selective MRN-Coronal MIP (inverted grey scale contrast) from a 3D DTI using single shot EPI (b value 0, 800, 1000 s/mm2 and 12 directions of interrogation) shows the symmetrical normal appearance of bilateral brachial plexuses (arrows). However, notice the decrease in SNR as compared to diffusion weighted imaging as shown in Figure 5.
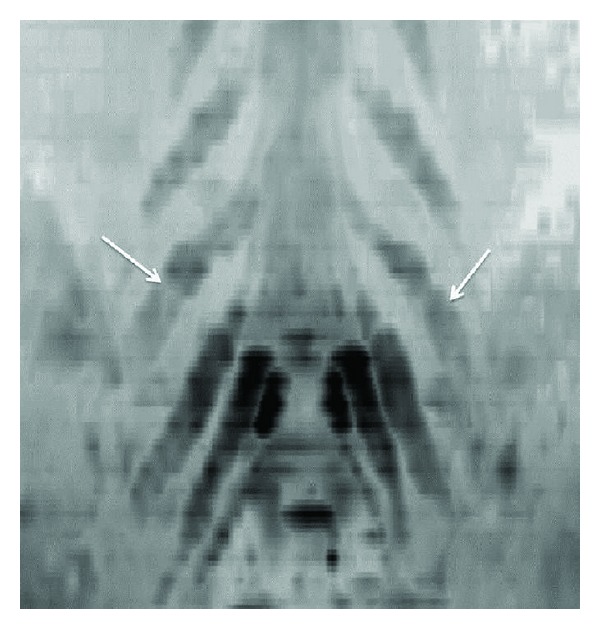
3D functional nerve selective MRN-Coronal MIP (inverted grey scale contrast) from a 3D DTI using single shot EPI (b values 0, 600 s/mm2 and 20 directions of interrogation) shows the symmetrical enlargement of bilateral LS plexus nerve roots (arrows) in a known case of hereditary motor and sensory neuropathy with diffusely reduced FA values in bilateral nerves.
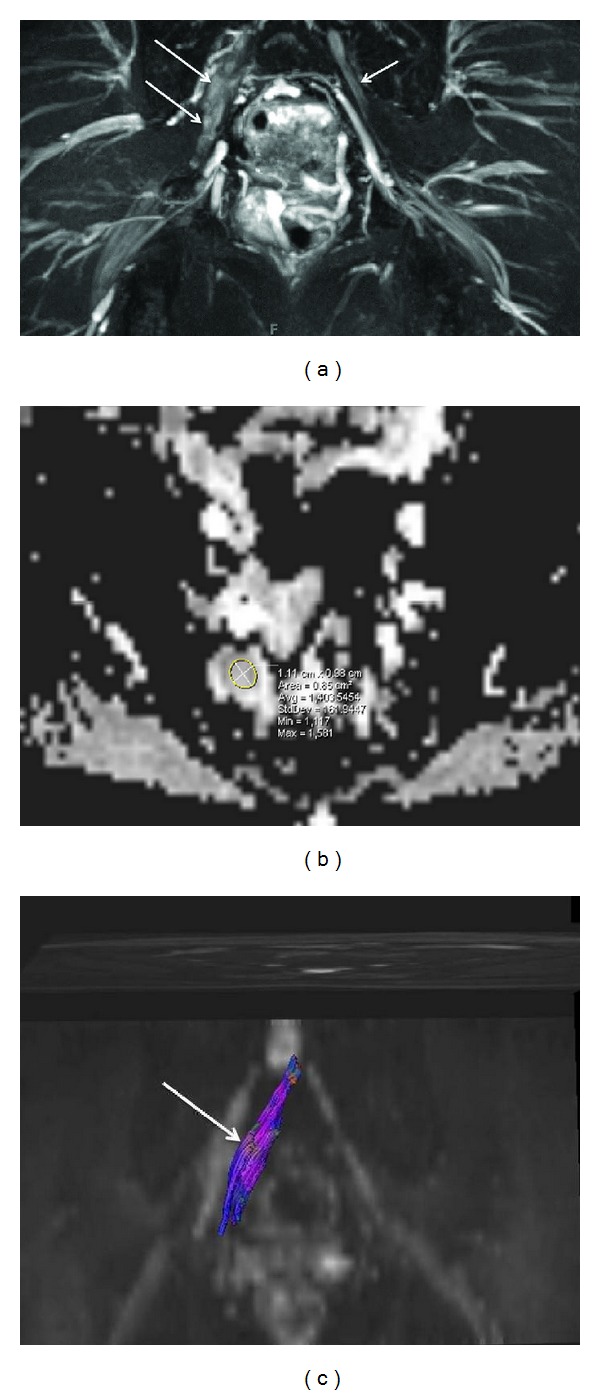
(a) Combined anatomic and functional MRN-MIP reconstruction from a 3D STIR SPACE sequence shows abnormal fusiform enlargement of the right S1 nerve root by a benign peripheral nerve sheath tumor (large arrows). Notice the normal appearance of the contralateral S1 nerve root (small arrow). (b) Combined anatomic and functional MRN-ADC map from single shot EPI DTI (b value 0, 600 s/mm2 and 20 directions) sequence shows high ADC value (1.4 × 10−3 mm2/s). (c) Combined anatomic and functional MRN-Tractography map following tensor calculation from single shot EPI DTI sequence shows nearly normal tracts (arrow) through the mass lesion in keeping with benign nature of the lesion.
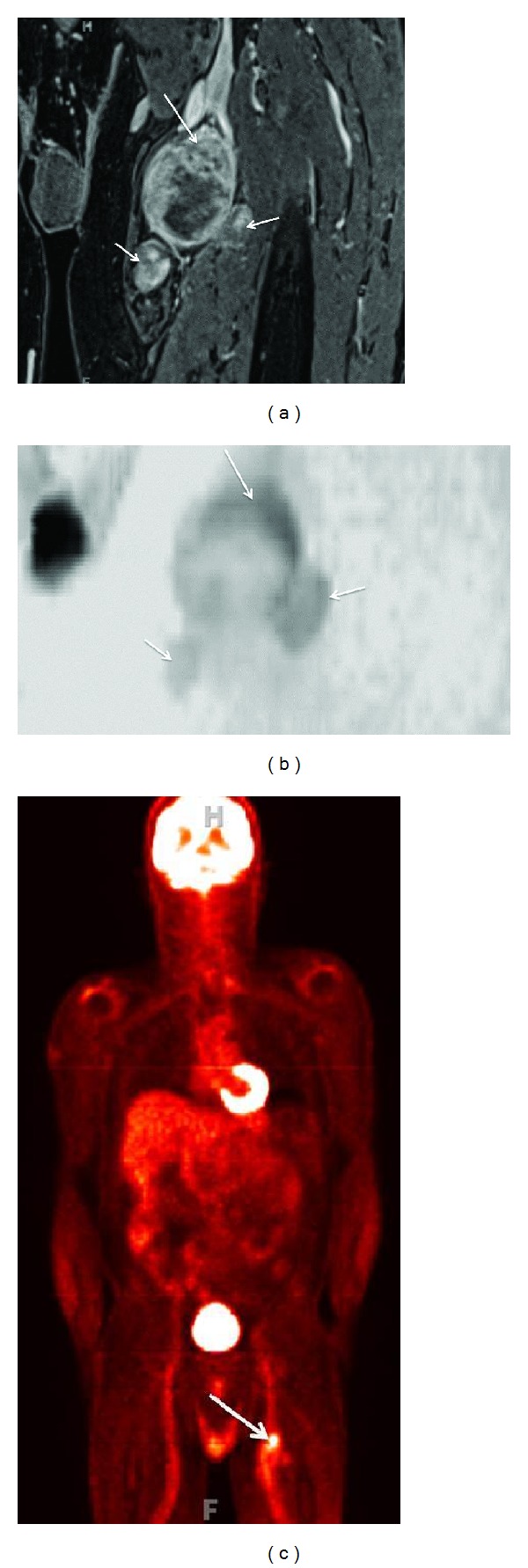
(a) Anatomic MRN, functional MRN, and F-18 FDG-PET correlation-Coronal fat suppressed postcontrast 3D T1W image of a biopsy proven malignant peripheral nerve sheath tumor shows the solid heterogeneous enhancement along the superior aspect of the lesion (large arrow). Notice additional smaller benign PNSTs in this case of neurofibromatosis type I (small arrows). (b) Anatomic MRN, functional MRN, and F-18 FDG-PET correlation-Coronal MIP reconstruction (inverted grey scale contrast) from single shot DTI (b values 0, 800, 1000 s/mm2, 12 directions) image shows the lowest ADC values (0.7 × 10−3 mm2/s) along the superior aspect of the lesion, which was targeted for the successful biopsy (large arrow). Notice that the additional smaller benign PNSTs show higher ADC values (small arrows). (c) Anatomic MRN, functional MRN, and F-18 FDG-PET correlation-Coronal F-18 FDG image shows high SUV max value (4 increased to 6 on delayed image) in the corresponding superior aspect of the lesion.
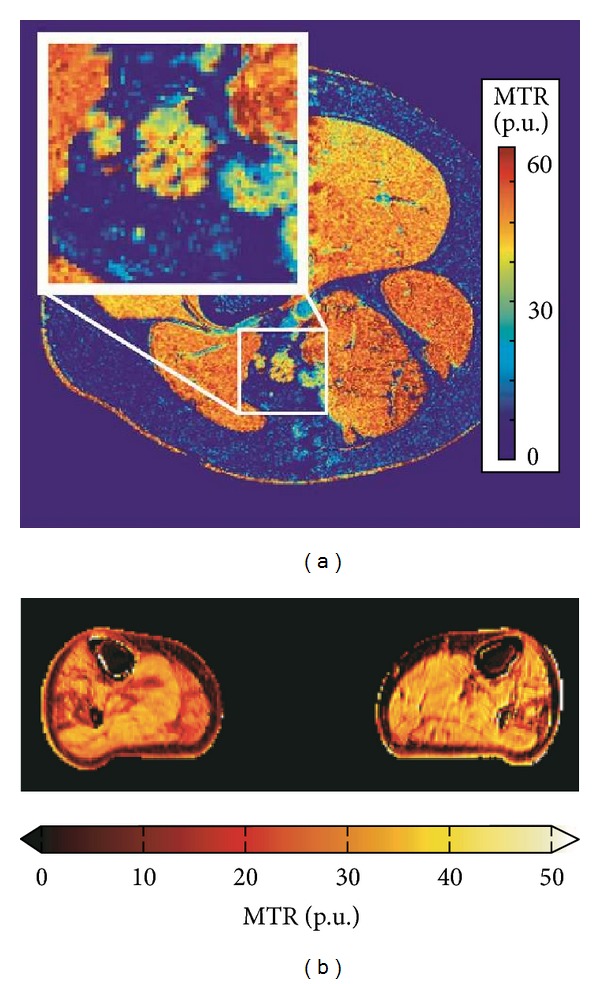
(a) MT neurography imaging of the sciatic nerve- Magnetization transfer ratio map at the mid-thigh level. Inset: enlargement of the sciatic nerve demonstrates measurable MTR effect in the nerve. (b) MT muscle imaging of neuropathy. Magnetization transfer ratio map of the mid-calf muscles of a patient with Charcot-Marie-Tooth disease type 1A (CMT1A). The MTR is reduced in areas affected by pathology. The maps have been corrected for RF inhomogeneities with a compensation method using B1 transmit maps [23].
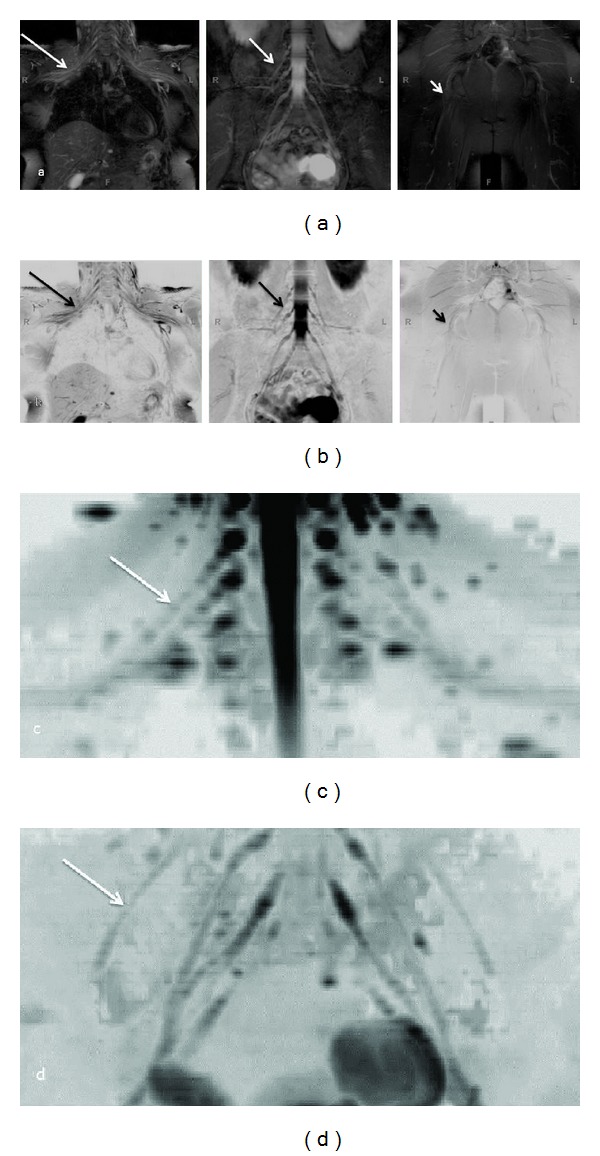
(a), (b) Whole body MRN: Coronal MIP reconstructions from 3D STIR SPACE sequence ((a) conventional window setting; (b) inverted window setting) show the normal appearance of bilateral brachial plexus (large arrows), LS plexus (medium arrows), and sciatic nerves (small arrows). (c), (d) Whole body MRN: Coronal MIP reconstructions (inverted grey scale contrast) from single shot DTI sequence (b values 0, 600 s/mm2, 20 directions) of the brachial plexus (c) and LS plexus (d).
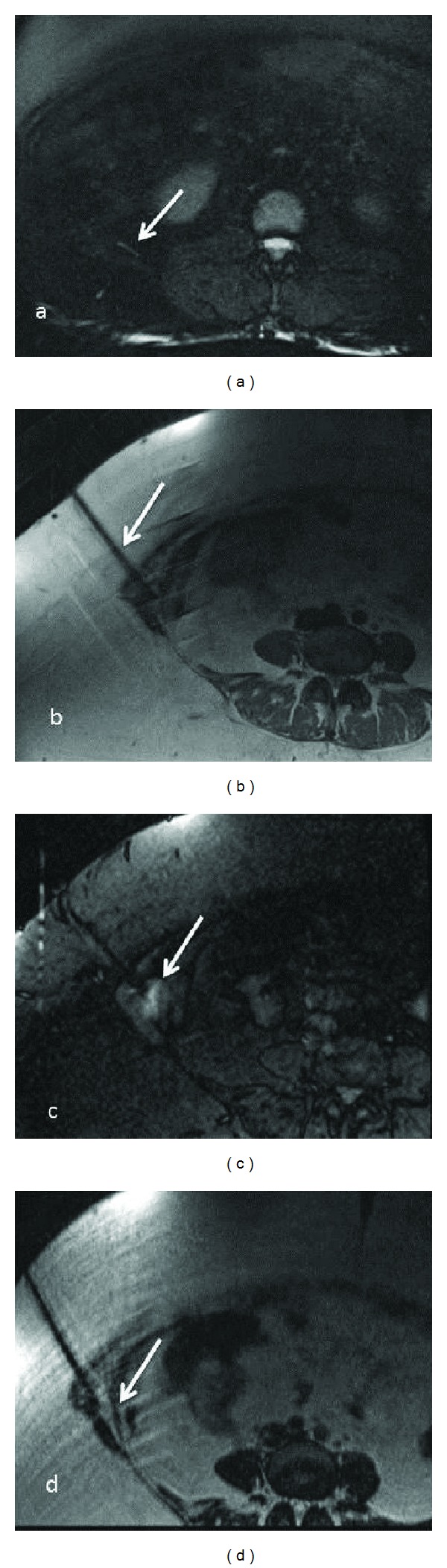
(a)–(d) MRN guided intervention-Axial T2 SPAIR (a), PDW (b), STIR (c), and T2 SPACE (d) images obtained during injection of local anesthetic and steroid combination around the right ilioinguinal nerve (arrow in a), beneath the external oblique aponeurosis. The patient experienced no significant pain relief following the injection in keeping with a negative block.
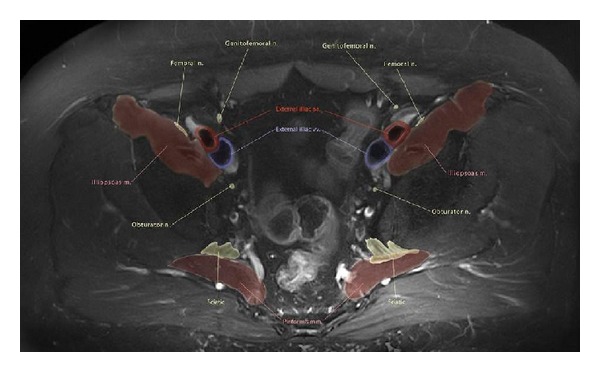
Anatomic illustration using MRN-Axial T2 SPAIR image through the upper pelvis with color drawing overlay nicely depicting the pelvic neuromuscular anatomy.
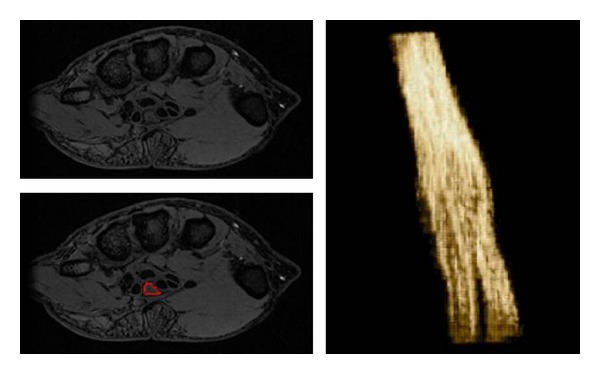
Nerve segmentation-Median nerve segmentation using custom made software. The tool allows semiautomated nerve segmentation, while a user draws region of interest on the nerve on sequential axial images.
References
-
- Viallon M, Vargas MI, Jlassi H, Lövblad KO, Delavelle J. High-resolution and functional magnetic resonance imaging of the brachial plexus using an isotropic 3D T2 STIR (Short Term Inversion Recovery) SPACE sequence and diffusion tensor imaging. European Radiology. 2008;18(5):1018–1023. - PubMed
-
- Zhang Z, Song L, Meng Q, et al. Morphological analysis in patients with sciatica: a magnetic resonance imaging study using three-dimensional high-resolution diffusion-weighted magnetic resonance neurography techniques. Spine. 2009;34(7):E245–E250. - PubMed
-
- Chhabra A, Andreisek G, Soldatos T, et al. MR neurography: past, present, and future. American Journal of Roentgenology. 2011;197:583–591. - PubMed
-
- Guggenberger R, Eppenberger P, Markovic D, et al. MR neurography of the median nerve at 3. 0T: optimization of diffusion tensor imaging and fiber tractography. European Journal of Radiology. 2012;81(7):e775–e782. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
