

Visitation policies and practices in US ICUs
- PMID: 23591058
- PMCID: PMC4056772
- DOI: 10.1186/cc12677
Visitation policies and practices in US ICUs
Abstract
Introduction: Prior reports suggest that restrictive ICU visitation policies can negatively impact patients and their loved ones. However, visitation practices in US ICUs, and the hospital factors associated with them, are not well described.
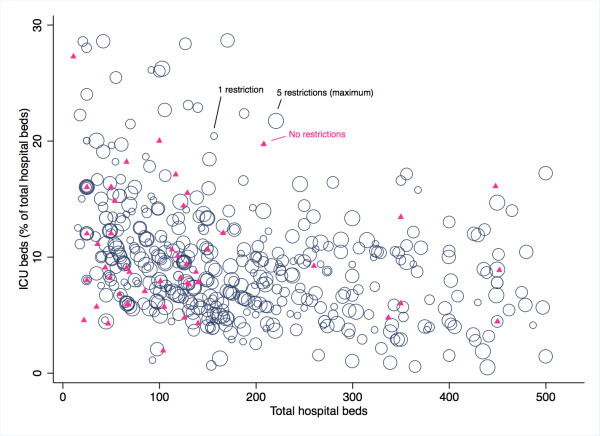
Methods: A telephone survey was made of ICUs, stratified by US region and hospital type (community, federal, or university), between 2008 and 2009. Hospital characteristics were self-reported and included the hospitals' bed number, critical care unit number, and presence of ICU leadership. Hospital and ICU visitation restrictions were based on five criteria: visiting hours; visit duration; number of visitors; age of visitors; and membership in the patient's immediate family. Hospitals or ICUs without restrictions had open visitation policies; those with any restriction had restrictive policies.
Results: The study surveyed 606 hospitals in the Northeast (17.0%), Midwest (26.2%), South (36.6%), and West (20.1%) regions; most were community hospitals (n = 401, 66.2%). The mean hospital size was 239 ± 217 beds; the mean percentage of ICU beds was 11.6% ± 13.4%. Hospitals often had restrictive hospital (n = 463, 76.4%) and ICU (n = 543, 89.6%) visitation policies. Many ICUs had ≥ 3 restrictions (n = 375; 61.9%), most commonly related to visiting hours and visitor number or age. Nearly all ICUs allowed visitation exceptions (n = 474; 94.8%). ICUs with open policies were more common in hospitals with < 150 beds. Among restrictive ICUs, the bed size, hospital type, number of critical care units, and ICU leadership were not associated with the number of restrictions. On average, hospitals in the Midwest had the least restrictive policies, while those in the Northeast had the most restrictive.
Conclusion: In 2008 the overwhelming majority of US ICUs in this study had restrictive visitation policies. Wide variability in visitation policies suggests that further study into the impact of ICU visitations on care and outcomes remains necessary to standardize practice.
Figures
Comment in
-
Open visitation policies and practices in US ICUs: can we ever get there?Crit Care. 2013 Jul 31;17(4):171. doi: 10.1186/cc12763. Crit Care. 2013. PMID: 23905784 Free PMC article.
References
-
- Angus DC, Carlet J. Surviving intensive care: a report from the 2002 Brussels Roundtable. Intensive Care Med. 2003;17:368–377. - PubMed
-
- Needham DM, Davidson J, Cohen H, Hopkins RO, Weinert C, Wunsch H, Zawistowski C, Bemis-Dougherty A, Berney SC, Bienvenu OJ, Brady SL, Brodsky MB, Denehy L, Elliott D, Flatley C, Harabin AL, Jones C, Louis D, Meltzer W, Muldoon SR, Palmer JB, Perme C, Robinson M, Schmidt DM, Scruth E, Spill GR, Storey CP, Render M, Votto J, Harvey MA. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders' conference. Crit Care Med. 2012;17:502–509. doi: 10.1097/CCM.0b013e318232da75. - DOI - PubMed
-
- Davidson JE, Powers K, Hedayat KM, Tieszen M, Kon AA, Shepard E, Spuhler V, Todres ID, Levy M, Barr J, Ghandi R, Hirsch G, Armstrong D. American College of Critical Care Medicine Task Force 2004-2005, Society of Critical Care Medicine. Clinical practice guidelines for support of the family in the patient-centered intensive care unit: American College of Critical Care Medicine Task Force 2004-2005. Crit Care Med. 2007;17:605–622. doi: 10.1097/01.CCM.0000254067.14607.EB. - DOI - PubMed
-
- The Joint Commission. Advancing Effective Communication, Cultural Competence, and Patient- and Family-centered Care: A Roadmap for Hospitals. Oakbrook Terrace, IL: The Joint Commission; 2010.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
