

High-resolution spectral domain anterior segment optical coherence tomography in type 1 Boston keratoprosthesis
- PMID: 23591146
- PMCID: PMC3741091
- DOI: 10.1097/ICO.0b013e318285c8f4
High-resolution spectral domain anterior segment optical coherence tomography in type 1 Boston keratoprosthesis
Abstract
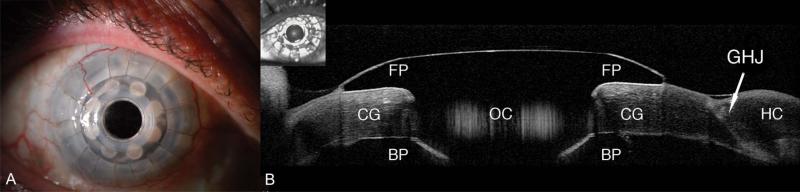
Purpose: To report the results of imaging using high-resolution, Fourier domain anterior segment optical coherence tomography (AS-OCT) to evaluate patients with a type 1 Boston Keratoprosthesis (KPro).
Methods: We performed a retrospective comparative study of patients in whom we implanted the Boston KPro. A total of 26 eyes of 23 patients from the Cornea Service at the University of California Davis Eye Center were included. Subjects were evaluated with the Spectralis AS-OCT (Heidelberg Engineering GmbH).
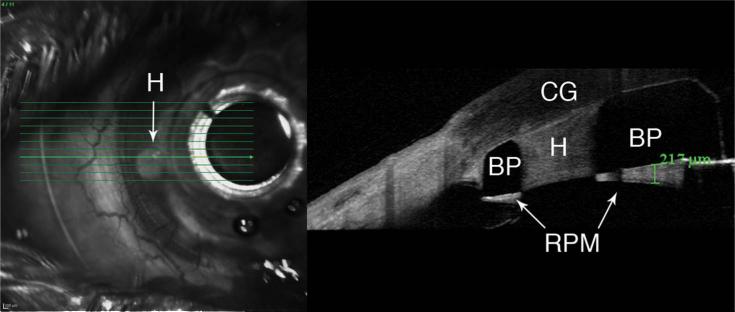
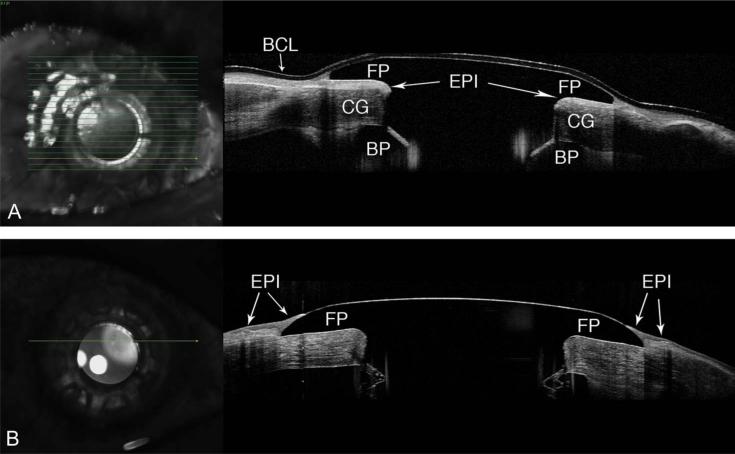
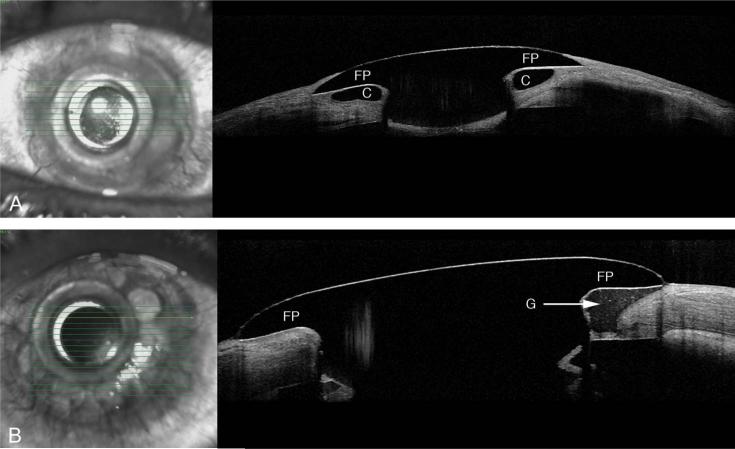
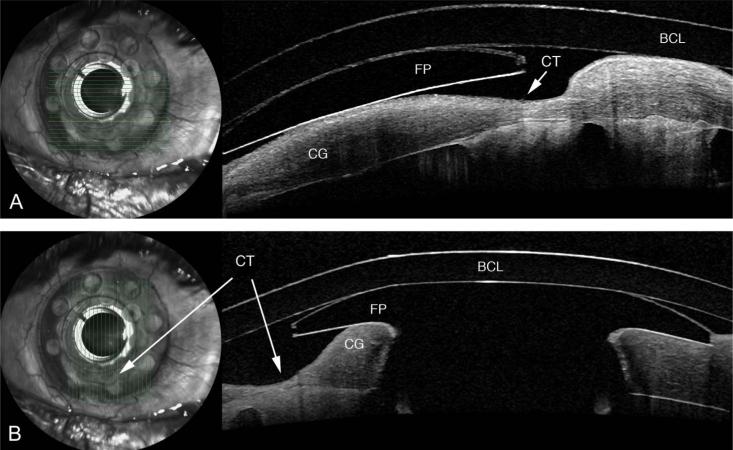
Results: Preoperative diagnoses for KPro surgery included failed corneal transplant (69%), chemical burn (23%), and aniridia (8%). The average age of patients was 63.2 years (range, 17-88 years). Fifty-four percent of the patients were female. The mean duration between the KPro surgery and the acquisition of high-resolution AS-OCT imaging was 35.8 months (range, 2-90 months). The most commonly observed finding was retroprosthetic membrane formation, which we found in 77% of KPro eyes. In 65% of KPro eyes, we identified epithelium behind the front plate, and in 54%, we identified an epithelial lip over the anterior surface of the KPro front plate. In 31% of KPro eyes, we identified periprosthetic cysts, gaps or spaces, and thinning in the corneal carrier graft.
Conclusions: Fourier domain AS-OCT is a useful noninvasive imaging technique in patients with a KPro and provides the ability to identify changes that are sometimes difficult to appreciate by clinical evaluation. The higher resolution Fourier domain systems may aid in the clinical diagnosis and management of pathology that might not be imaged with instruments of lower resolution. AS-OCT has the potential for monitoring the anatomic stability of an implanted KPro and may also help to monitor for complications. Moreover, high-resolution imaging may enhance our understanding of periprosthetic anatomy.
Figures
References
-
- Dohlman CH, Doane MG. Some factors influencing outcome after keratoprosthesis surgery. Cornea. 1994;13:214–218. - PubMed
-
- Doane MG, Dohlman CH, Bearse G. Fabrication of a keratoprosthesis. Cornea. 1996;15:179–184. - PubMed
-
- Tugal-Tutkun I, Akova YA, Foster CS. Penetrating keratoplasty in cicatrizing conjunctival diseases. Ophthalmology. 1995;102:576–585. - PubMed
-
- Soong HK. Penetrating keratoplasty in ocular surface disease. In: Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea: Surgery of the Cornea and Conjunctiva. Mosby; St Louis, MO: 1997. pp. 1781–1788.
-
- Yaghouti F, Dohlman CH. Innovations in keratoprosthesis: proved and unproved. Int Ophthalmol Clin. 1999;39:27–36. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
