

Increasing critical care admissions from U.S. emergency departments, 2001-2009
- PMID: 23591207
- PMCID: PMC3756824
- DOI: 10.1097/CCM.0b013e31827c086f
Increasing critical care admissions from U.S. emergency departments, 2001-2009
Abstract
Objectives: Little is known about how recent system-wide increases in demand for critical care have affected U.S. emergency departments (EDs). This study describes changes in the amount of critical care provided in U.S. EDs between 2001 and 2009.
Design: Analysis of data from the National Hospital Ambulatory Medical Care Survey for the years 2001-2009.
Setting: National multistage probability sample of U.S. ED data. U.S. ED capacity was estimated using the National Emergency Department Inventory-United States.
Patients: : ED patients admitted a critical care unit.
Interventions: None.
Measurements: Annual hours of ED-based critical care and annual number critical care ED visits. Clinical characteristics, demographics, insurance status, setting, geographic region, and ED length of stay for critically ill ED patients.
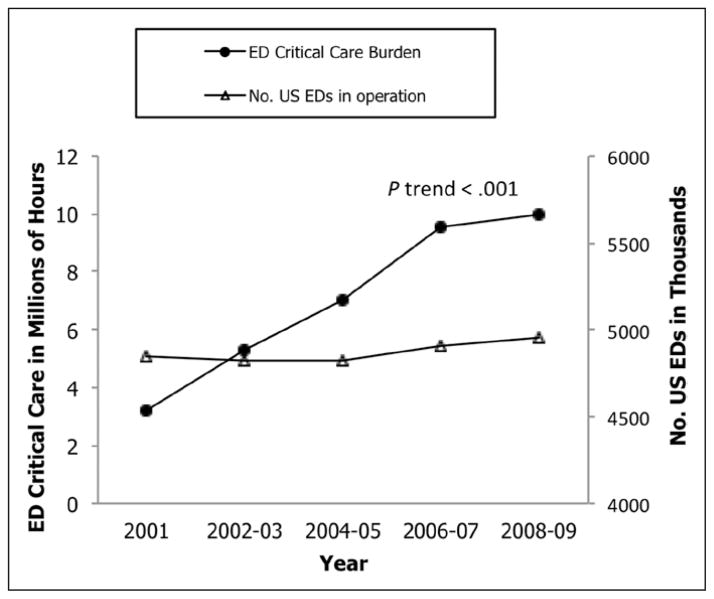
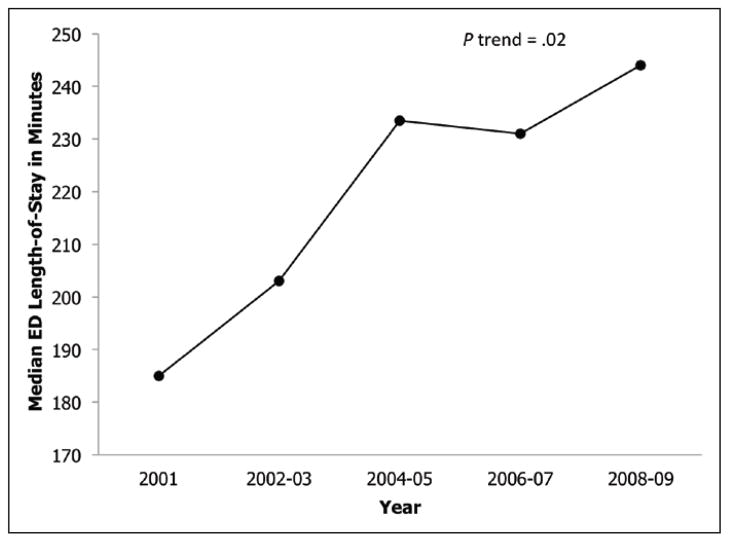
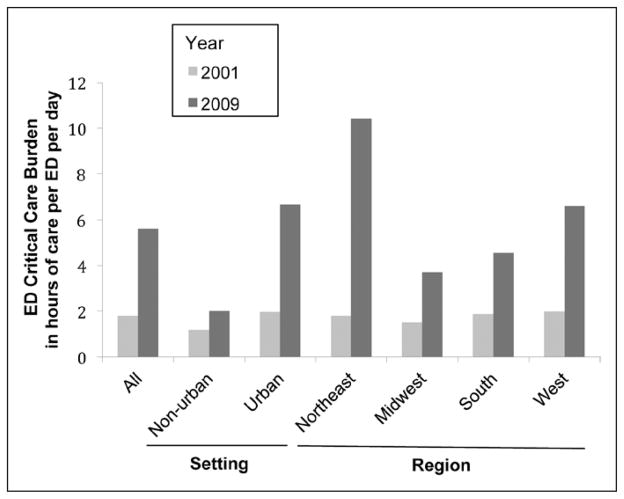
Main results: Annual critical care unit admissions from U.S. EDs increased by 79% from 1.2 to 2.2 million. The proportion of all ED visits resulting in critical care unit admission increased from 0.9% to 1.6% (ptrend < 0.001). Between 2001 and 2009, the median ED length of stay for critically ill patients increased from 185 to 245 minutes (+ 60 min; ptrend < 0.02). For the aggregated years 2001-2009, ED length of stay for critical care visits was longer among black patients (12.6% longer) and Hispanic patients (14.8% longer) than among white patients, and one third of all critical care ED visits had an ED length of stay greater than 6 hrs. Between 2001 and 2009, total annual hours of critical care at U.S. EDs increased by 217% from 3.2 to 10.1 million (ptrend < 0.001). The average daily amount of critical care provided in U.S. EDs tripled from 1.8 to 5.6 hours per ED per day.
Conclusions: The amount of critical care provided in U.S. EDs has increased substantially over the past decade, driven by increasing numbers of critical care ED visits and lengthening ED length of stay. Increased critical care burden will further stress an already overcapacity U.S. emergency care system.
Conflict of interest statement
Dr. Maselli received funding from the CDC. The remaining authors have not disclosed any potential conflicts of interest.
Figures
Comment in
-
Critical care in the emergency department: it's critical to know what's going on!Crit Care Med. 2013 May;41(5):1367-8. doi: 10.1097/CCM.0b013e318283d161. Crit Care Med. 2013. PMID: 23591216 No abstract available.
References
-
- Rivers EP, Nguyen HB, Huang DT, et al. Critical care and emergency medicine. Curr Opin Crit Care. 2002;8:600–606. - PubMed
-
- Halpern NA, Pastores SM. Critical care medicine in the United States 2000–2005: An analysis of bed numbers, occupancy rates, payer mix, and costs. Crit Care Med. 2010;38:65–71. - PubMed
-
- Halpern NA. Can the costs of critical care be controlled? Curr Opin Crit Care. 2009;15:591–596. - PubMed
-
- U.S. Department of Health and Human Services. Health Resources and Services Administration Report to Congress: The critical care workforce. [Accessed June 14, 2011];A study of the supply and demand for critical care physicians. Available at: http://bhpr.hrsa.gov/healthworkforce/reports/studycriticalcarephys.pdf.
-
- Angus DC, Kelley MA, Schmitz RJ, et al. Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: Can we meet the requirements of an aging population? JAMA. 2000;284:2762–2770. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
