

Does opioid pain medication use affect the outcome of patients with lumbar disc herniation?
- PMID: 23591657
- PMCID: PMC3718295
- DOI: 10.1097/BRS.0b013e3182959e4e
Does opioid pain medication use affect the outcome of patients with lumbar disc herniation?
Abstract
Study design: Subgroup analysis of prospective, randomized cohort.
Objective: To review the results of patients who received opioid pain medications during treatment compared with that of patients who did not receive opioid medications.
Summary of background data: The Spine Patient Outcomes Research Trial (SPORT) is a prospective, multicenter study of surgical treatment versus nonoperative treatment for lumbar intervertebral disc herniation.
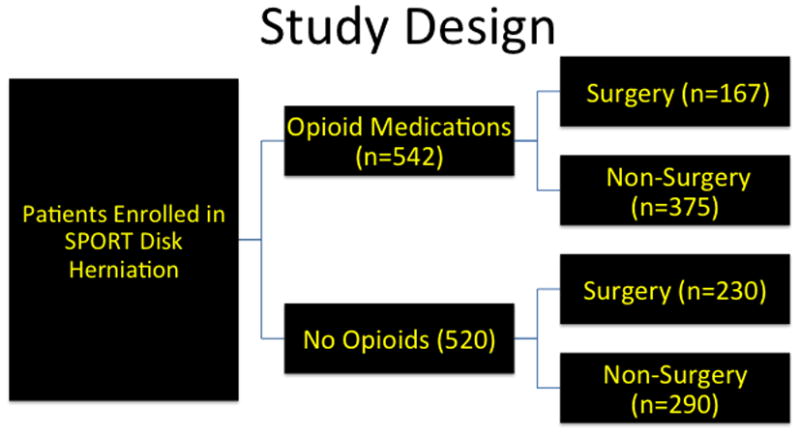
Methods: The study population includes patients enrolled in SPORT for treatment of intervertebral disc herniation in combined randomized and observational cohorts. Patients who received opioid medications at baseline (opioid) were compared with those who did not (nonopioid).
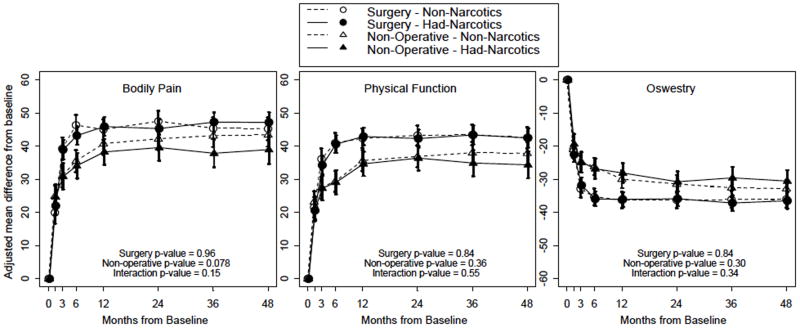
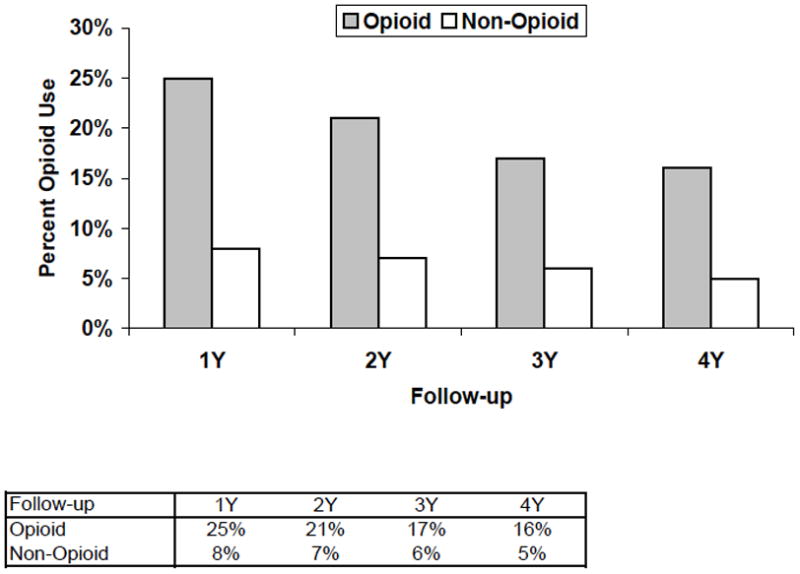
Results: There were 520 patients in the nonopioid group and 542 patients in the opioid group. Among the opioid medication group, there were significantly (P < 0.001) worse baseline scores in primary and secondary outcome measures. There was an increased percentage of patients in the opioid medication group with the perception of worsening symptoms and neurological deficit (P < 0.001). A higher percentage of the opioid group patients received surgery (P < 0.001).At 4 years of follow-up, there were no significant differences in primary or secondary outcome measures or treatment effect of surgery between opioid and nonopioid medication group patients. Opioid medications were associated with increased crossover to surgical treatment (P = 0.005) and decreased surgical avoidance (P = 0.01). The incidence of opioid use at 4 years was 16% among patients who were using opioids at baseline and 5% among patients who were not using opioids at baseline.
Conclusion: Patients who were treated with opioids had significantly worse baseline pain and quality of life. At final follow-up, there was no long-term difference in outcome associated with opioid pain medication use. Opioid medications were not associated with surgical avoidance. The majority of patients who use opioids during the study did not continue usage at 4 years.
Level of evidence: 2.
Figures
Similar articles
-
Systematic Review of Outcomes Following 10-Year Mark of Spine Patient Outcomes Research Trial for Intervertebral Disc Herniation.Spine (Phila Pa 1976). 2020 Jun 15;45(12):825-831. doi: 10.1097/BRS.0000000000003400. Spine (Phila Pa 1976). 2020. PMID: 32004232
-
Duration of symptoms resulting from lumbar disc herniation: effect on treatment outcomes: analysis of the Spine Patient Outcomes Research Trial (SPORT).J Bone Joint Surg Am. 2011 Oct 19;93(20):1906-14. doi: 10.2106/JBJS.J.00878. J Bone Joint Surg Am. 2011. PMID: 22012528 Free PMC article. Clinical Trial.
-
Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial.Spine (Phila Pa 1976). 2014 Jan 1;39(1):3-16. doi: 10.1097/BRS.0000000000000088. Spine (Phila Pa 1976). 2014. PMID: 24153171 Free PMC article. Clinical Trial.
-
Prediction based on preoperative opioid use of clinical outcomes after transforaminal lumbar interbody fusions.J Neurosurg Spine. 2017 Feb;26(2):144-149. doi: 10.3171/2016.7.SPINE16284. Epub 2016 Sep 30. J Neurosurg Spine. 2017. PMID: 27689425 Clinical Trial.
-
Patient preferences and expectations for care: determinants in patients with lumbar intervertebral disc herniation.Spine (Phila Pa 1976). 2008 Nov 15;33(24):2663-8. doi: 10.1097/BRS.0b013e31818cb0db. Spine (Phila Pa 1976). 2008. PMID: 18981962 Free PMC article. Clinical Trial.
Cited by
-
Conservative treatments for lumbar radicular pain.Curr Pain Headache Rep. 2014 Oct;18(10):452. doi: 10.1007/s11916-014-0452-1. Curr Pain Headache Rep. 2014. PMID: 25230798 Review.
-
Which Variables Are Associated With Patient-reported Outcomes After Discectomy? Review of SPORT Disc Herniation Studies.Clin Orthop Relat Res. 2015 Jun;473(6):2000-6. doi: 10.1007/s11999-014-3671-1. Clin Orthop Relat Res. 2015. PMID: 24818737 Free PMC article. Review.
-
Predictors of Prolonged Opioid Use After Lumbar Fusion and the Effects of Opioid Use on Patient-Reported Outcome Measures.Global Spine J. 2021 Sep 6;13(6):21925682211041968. doi: 10.1177/21925682211041968. Online ahead of print. Global Spine J. 2021. PMID: 34488470 Free PMC article.
-
Lumbar disc herniation: what has the Spine Patient Outcomes Research Trial taught us?Int Orthop. 2019 Apr;43(4):853-859. doi: 10.1007/s00264-019-04309-x. Epub 2019 Feb 15. Int Orthop. 2019. PMID: 30767043 Review.
-
Opioid use prior to surgery is associated with worse preoperative and postoperative patient reported quality of life and decreased surgical cost effectiveness for symptomatic adult spine deformity; A matched cohort analysis.N Am Spine Soc J. 2021 Dec 12;9:100096. doi: 10.1016/j.xnsj.2021.100096. eCollection 2022 Mar. N Am Spine Soc J. 2021. PMID: 35141660 Free PMC article.
References
-
- Olsen Y, Daumit GL, Ford DE. Opioid prescriptions by U.S. primary care physicians from 1992 to 2001. The journal of pain: official journal of the American Pain Society. 2006;7(4):225–35. - PubMed
-
- Birnbaum HG, et al. Estimated costs of prescription opioid analgesic abuse in the United States in 2001: a societal perspective. The Clinical journal of pain. 2006;22(8):667–76. - PubMed
-
- Colliver JD, KL, Dai L, Gfroerer JC. Misuse of Prescription Drugs: Data from the 2002, 2003, and 2004 National Surveys on Drug Use and Health. Vol. 2006. Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2006. Prevalence and recent trends in misuse of prescription drugs. DHHS publication no. SMA 06–4192(Analytic Series A-28.)
-
- Angst MS, Clark JD. Opioid-induced hyperalgesia: a qualitative systematic review. Anesthesiology. 2006;104(3):570–87. - PubMed
-
- Mao J, Mayer DJ. Spinal cord neuroplasticity following repeated opioid exposure and its relation to pathological pain. Annals of the New York Academy of Sciences. 2001;933:175–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
