

Hepatobiliary anomalies associated with ABCB4/MDR3 deficiency in adults: a pictorial essay
- PMID: 23591976
- PMCID: PMC3675252
- DOI: 10.1007/s13244-013-0243-y
Hepatobiliary anomalies associated with ABCB4/MDR3 deficiency in adults: a pictorial essay
Abstract
Background: ABCB4/MDR3 gene variants are mostly associated with a peculiar form of cholelithiasis in European adults, currently referred to as low phospholipid-associated cholelithiasis (LPAC) syndrome.
Methods: LPAC syndrome is a rare genetic disorder, characterised by the following clinical features: biliary symptoms before the age of 40, recurrence of the symptoms after cholecystectomy, and intrahepatic microlithiasis or intrahepatic hyperechogenic foci.
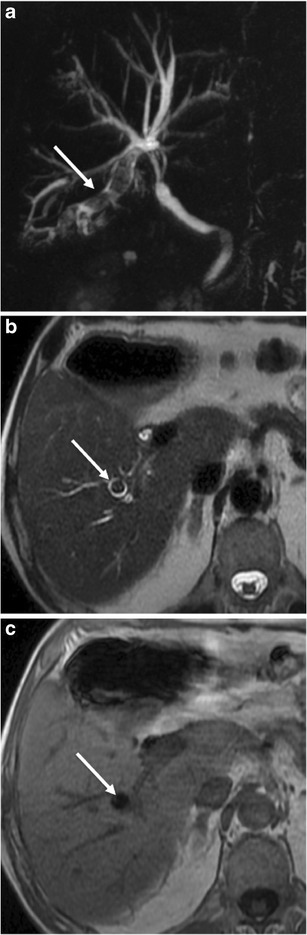
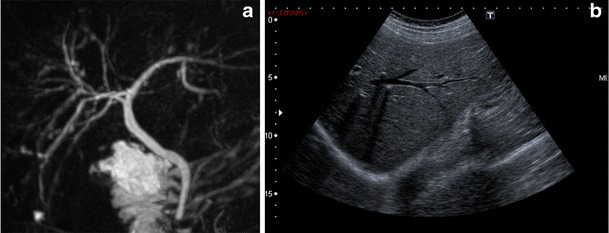
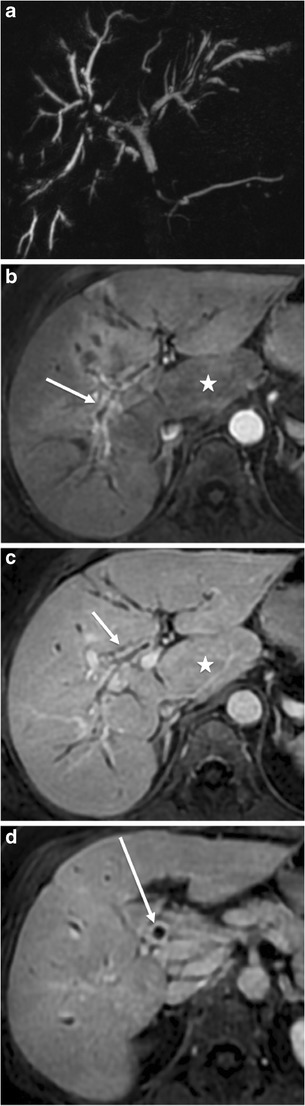
Results: Imaging features associated with ABCB4/MDR3 mutations are not specific and correspond to a wide spectrum of biliary abnormalities. The main feature is the presence of intrahepatic lithiasis. Other uncommon presentations have been described, such as uni- or multifocal spindle-shaped dilatations of the intrahepatic bile ducts filled with gallstones, secondary sclerosing cholangitis, biliary cirrhosis, and intrahepatic cholangiocarcinoma.
Conclusion: This review focuses on MR features related to ABCB4/MDR3 mutations.
Main messages: • LPAC syndrome is characterised by intrahepatic microlithiasis or intrahepatic hyperechogenic foci. • Ultrasound examination is very accurate in detecting intrahepatic stones. • At MR imaging, LPAC syndrome is associated with various presentations.
Figures








References
LinkOut - more resources
Full Text Sources
Other Literature Sources
